Article Text

Abstract
Introduction Gestational diabetes mellitus (GDM) is a common complication of pregnancy with implications for cardiovascular health. Among reproductive-aged women, less is known about nativity-related disparities in cardiometabolic risk profiles and GDM history. We examined how cardiometabolic risk profiles and GDM history differed by nativity and explored associations between acculturation, cardiometabolic risk profiles and GDM history.
Research design and methods We analyzed cross-sectional data from the 2016–2017 National Health Interview Survey among reproductive-aged women (18–49 years) who both reported ever being pregnant and answered the question on GDM history. Using multivariable logistic regression, we examined the percentage with GDM history and compared cardiometabolic profiles by nativity status and acculturation (duration of US residence).
Results Of 9525 women, 22.5% were foreign-born. Also, 11.7% of foreign-born women had a GDM history vs 9.6% of US-born women. Foreign-born women with ≥10 years US residence had the highest age-standardized percentage with GDM history (11.0%) compared with US-born women (9.2%) and foreign-born women with <10 years US residence (6.7%). US-born women had a higher prevalence of hypertension, current smoking, and alcohol use than foreign-born women. Among foreign-born women, those with ≥10 years US residence had a higher prevalence of hypertension, current smoking, and alcohol use than those with <10 years US residence. In the fully adjusted model, foreign-born women with ≥10 years US residence had higher odds of GDM history than US-born women (OR 1.43; 95% CI 1.17 to 1.76) while foreign-born women with <10 years US residence and US-born women has similar odds of GDM history.
Conclusions Greater duration of US residence may be associated with nativity-related disparities in GDM. Acculturation, including changing health-related behaviors may explain the disparities among foreign-born women and should be further investigated to appropriately target interventions to prevent GDM and future cardiometabolic diseases.
- diabetes
- gestational
- pregnancy
- health behavior
- healthcare disparities
Data availability statement
Data are available in a public, open access repository. The data used in this study are publicly available from the National Health Interview Survey (NHIS) website (https://www.cdc.gov/nchs/nhis/data-questionnaires-documentation.htm)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Gestational diabetes mellitus (GDM) disproportionally effects foreign-born (vs US-born) women.
What are the new findings?
In this sample of women of reproductive age, foreign-born women with shorter duration of US residence (<10 years) had lower prevalence of cardiometabolic risk factors than US-born women.
Foreign-born women with longer duration of US residence (≥10 years) had greater odds of GDM history than US-born women.
Foreign-born women with shorter duration of US residence (<10 years) and US-born women did not differ in their odds of GDM history.
How might these results change the focus of research or clinical practice?
With increasing duration of US residence, foreign-born women may adopt unhealthy behaviors which may impact maternal health outcomes—including risk of GDM.
Acculturation, including changing health-related behaviors should be further investigated to appropriately target interventions to reduce risk of GDM and future cardiometabolic diseases.
Clinicians should consider lifestyle patterns (ie, diet, physical activity)—which are heavily influenced by nativity and may change with acculturation—during preconception counseling to reduce the risk of GDM.
Background
Gestational diabetes mellitus (GDM) is defined as diabetes first diagnosed during pregnancy without pre-existing type 1 or type 2 diabetes mellitus.1 GDM complicates 6%–9% of pregnancies in the USA and is associated with significant adverse health outcomes for pregnant women and their infants.2 3 Compared with women without GDM, women with GDM are more likely to suffer from pre-eclampsia and require cesarean delivery.3 They are over seven times more likely to develop type 2 diabetes mellitus, and twice as likely to develop chronic hypertension, hyperlipidemia, and coronary artery disease.4–6 Similarly, infants born to mothers with GDM have an increased risk of being large-for-gestational-age, developing shoulder dystocia during delivery, and suffering postdelivery hypoglycemia.7 8
Despite diagnostic and therapeutic advances aimed at reducing the burden of GDM and related adverse outcomes, the prevalence of GDM continues to rise worldwide.9 This rise in GDM prevalence is likely related to the parallel rise in the prevalence of obesity and increases in average maternal age.3 10 11 These global trends are also apparent in the USA, where GDM prevalence has increased from 3.7% to 6% between 2010 and 2016.12
Similar to US trends for other adverse pregnancy outcomes, there are marked disparities in the prevalence of GDM by race and ethnicity.2 13 Asian, Hispanic, and black women are at an increased risk of developing GDM compared with non-Hispanic (NH) white women.14 15 Another critical risk factor for GDM is nativity or country of origin. Unlike many other perinatal health outcomes (eg, preterm birth, low birth weight, and pre-eclampsia) in which immigrant status appears to be protective for disease development, a phenomenon known as ‘the healthy immigrant effect’,16–18 the risk of GDM is higher among those born outside of the USA (hereafter referred to as foreign-born) compared with those born in the USA (hereafter referred to as US-born).19–22 The divergence in the risk of GDM among foreign-born women has been challenging to explain, given that traditional risk factors for GDM, such as obesity23 and harmful health behaviors (eg, westernized diet, sedentary lifestyle)24 tend to be lower among foreign-born women.22 25 26
It is possible that immigrant health deteriorates with a longer residence in the USA, partly due to the adoption of unhealthy behaviors.27–29 Acculturation, defined broadly as changes in culture, values, and practices when immigrants arrive in a new country,30 may help explain patterns of disease prevalence among immigrants. The demands of this adaptative process, including, but not limited to increased exposure to discrimination, have been linked with adverse mental health outcomes and cardiovascular disease risk.31–34 Proxies of acculturation, such as duration of US residence, have also been associated with worsening health behaviors and cardiometabolic health outcomes.35–38
However, to our knowledge, associations between acculturation, cardiometabolic health, and GDM history among reproductive-aged women who have immigrated to the USA, are not well examined. Using a nationally representative sample, we aimed to (1) examine how cardiometabolic risk profiles and GDM history differ between US-born and foreign-born women, and (2) examine differences in cardiometabolic risk profile and GDM history by duration of US residence (among foreign-born women).
Methods
Data source
We used data from the 2016–2017 National Health Interview Survey (NHIS), which was the first time since 2006 that a question on GDM was included. The NHIS is a cross-sectional, nationally representative study of civilian non-institutionalized US adults aged ≥18 years and is administered by the National Center for Health Statistics (NCHS).39 40 The NHIS uses a complex multistage probability sampling design which includes clustering and stratification.39 Before 2018, minority, elderly, and low-income individuals were oversampled in NHIS. Demographics, health indicators, and healthcare use data were obtained via in-person (face-to-face) interviews in English or Spanish. For NHIS, one adult per household is selected randomly and interviewed using the Sample Adult Module to provide detailed information on health status, health status, and use of healthcare services. All respondents provided oral informed consent. A detailed description of the design, methods, study materials, and analytic methods for the NHIS is published elsewhere.39 40 Our current study did not require review by an institutional review board because it used deidentified publicly accessible data published by NCHS.40
Study population
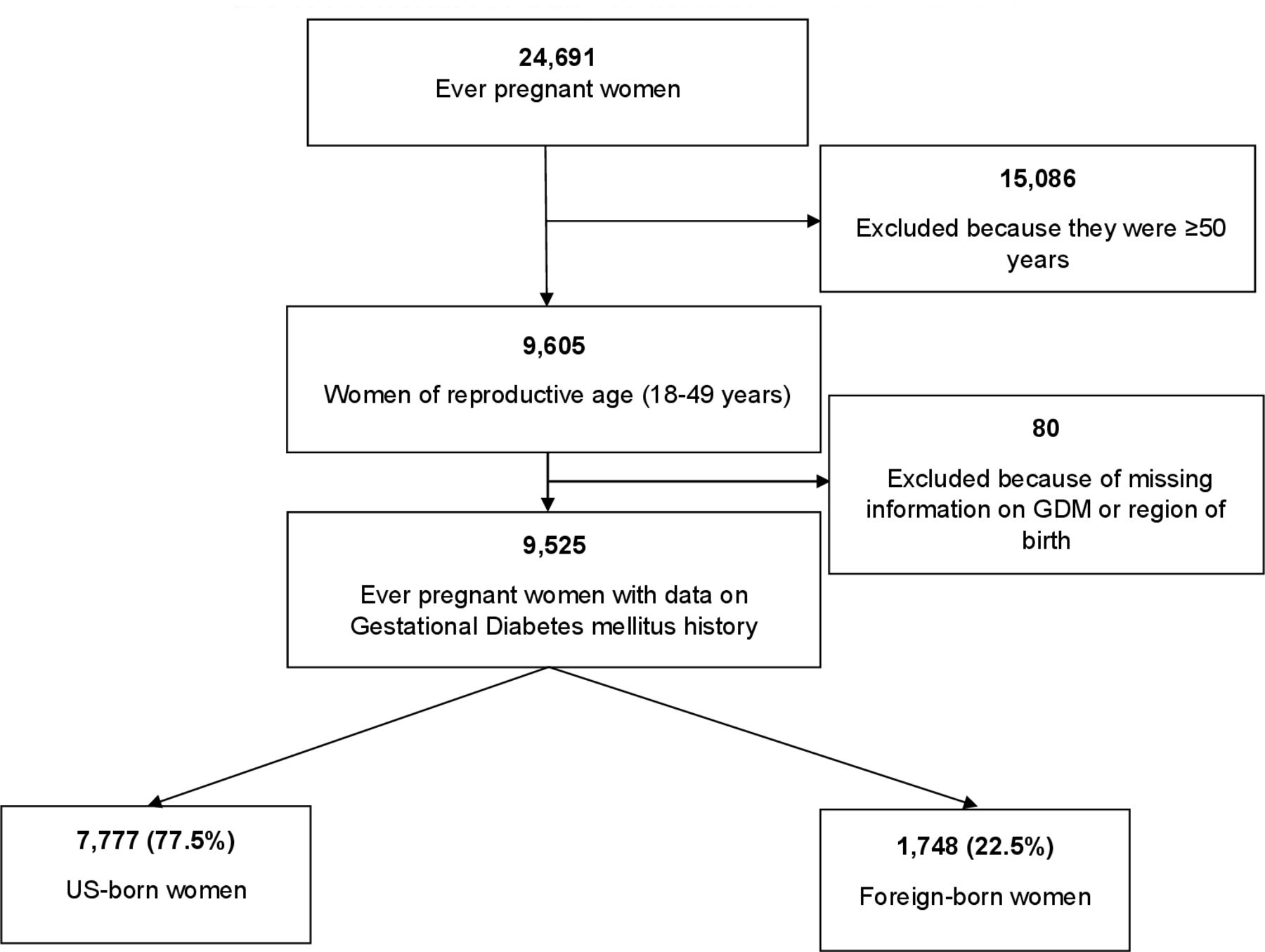
Women who were aged 18–49 years, an age group classified by WHO as being of reproductive age,41 who reported ever being pregnant and responded to the question on GDM history (median age 37, IQR 31–43) were included in the study sample. Women who self-identified as born in the USA by an affirmative response to the question: “Were you born in the United States?” were considered US-born. Women who were not born in any of the 50 US States or the District of Columbia were deemed to be foreign-born. These included those who were refugees, undocumented immigrants, on visas, including students or guest workers, naturalized citizens, and legal permanent residents.39 Information on respondents’ country of origin is restricted and was therefore not examined. The final study population included 7777 US-born women and 1748 foreign-born women (figure 1). Weighted to account for the complex sampling strategy and to produce estimates representative of the total US population, these sample sizes represent 3 129 880 and 772 210 of US-born and foreign-born women, respectively.
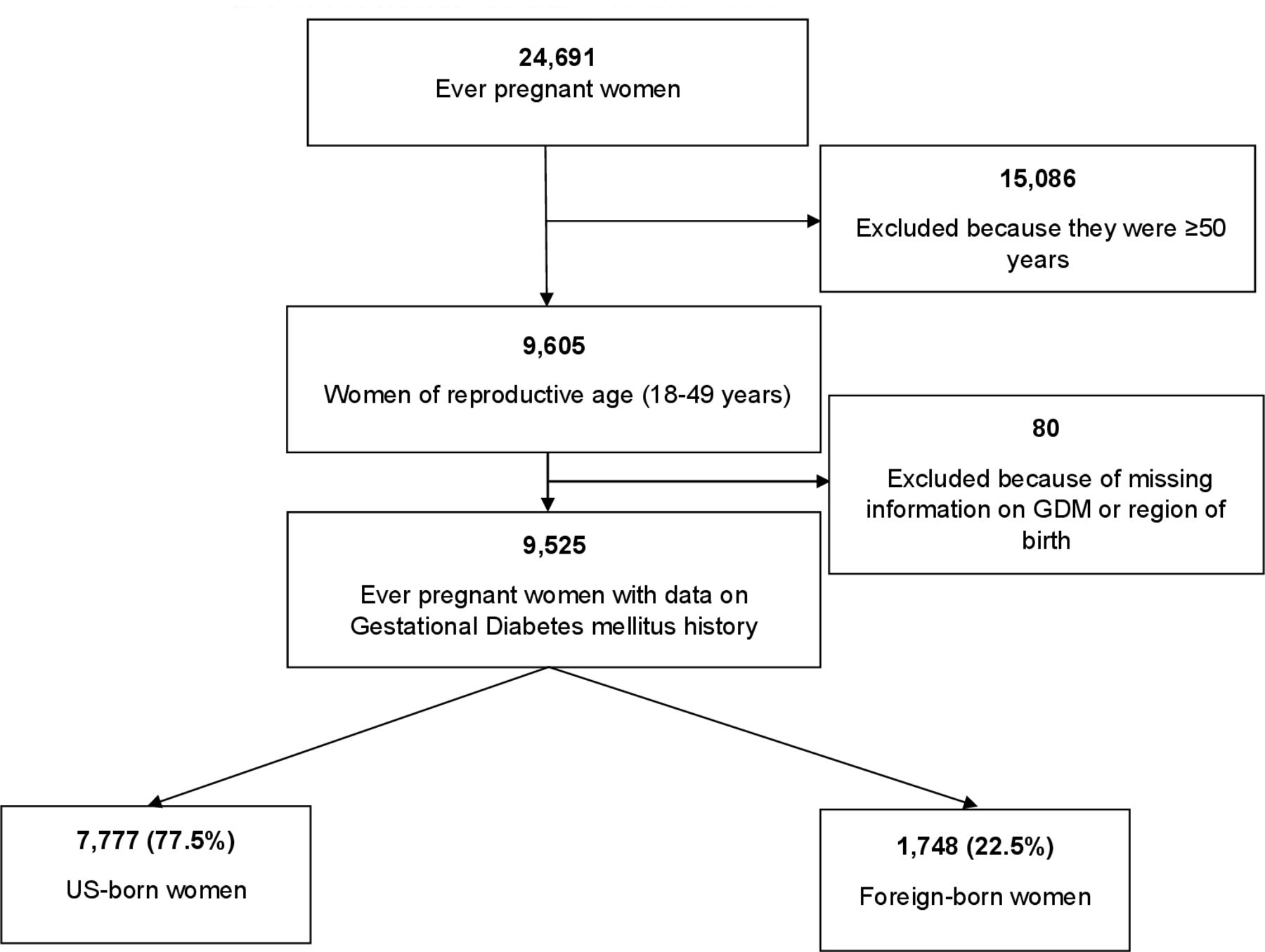
Flow chart of sample included in the analyses. GDM, gestational diabetes mellitus.
Outcome
The outcome of interest, GDM history, was defined as a self-reported affirmative response to the question: “Were you FIRST told by a doctor or other health professional that you had diabetes, sugar diabetes, or gestational diabetes during pregnancy?” While GDM history was not objectively validated in this study, prior studies report a high sensitivity and specificity of self-reported GDM.42
Covariates
Sociodemographic covariates for this study included age (at survey response), marital status, level of education, race/ethnicity, employment status, and health insurance status. We were unable to assess parity and age at GDM diagnosis because the NHIS does not include these questions in the survey. To assess the duration of US residence, persons born outside the USA were asked: “About how long have you been in the United States?” Responses to this question were categorized as <10 years and ≥10 years. The cut-off of 10 years was used because 10 or more years of stay in the USA has been used in prior studies measuring acculturation, and were associated with a higher prevalence of cardiometabolic disease risk factors in immigrants.37 43 44 Poverty-income ratio (PIR), defined as the ratio of a household’s income to poverty, is the ratio of the midpoint of a respondent’s family income divided by the poverty level for that year. The PIR was categorized into poor (PIR <1: below the federal poverty level), near-poor (PIR 1–2: between 100% and 200% of the federal poverty level), and not poor/near-poor (PIR ≥2: ≥200% above the federal poverty level).
Cardiometabolic risk profile factors examined included body mass index (BMI), which was calculated using respondents’ self-reported height and weight and based on the National Institute of Health (NIH) classifications.45 A BMI ≥25 kg/m2 in non-Asian respondents, and ≥23 kg/m2 for persons born in Asia, Southeast Asia, and on the Indian subcontinent was designated as overweight/obese and normal if otherwise, according to WHO guidelines.46 History of hypertension was assessed with the question: “Have you EVER been told by a doctor or other health professional that you had hypertension, also called high blood pressure?” Persons with affirmative responses were classified as having a history of hypertension. A current smoker was a participant who reported smoking ‘every day’ or ‘some days’ when asked: “Do you NOW smoke cigarettes every day, some days, or none at all?” among persons who had said yes to “ever smoked at least 100 cigarettes in [their] entire life”. For alcohol use, respondents who had never had at least 12 drinks in their lifetime were classified as never drinkers. Those who had at least 12 drinks in their lifetime but had no alcohol consumption in the past 12 months were former drinkers. Respondents who consumed at least 12 drinks in their lifetime and drank on at least 1 day in the past year were classified as current drinkers. Among the current drinkers, those who reported consuming <12 drinks in the past year to fewer than 3 drinks a week were considered current light drinkers and those who drank 3 or more drinks a week were considered current heavy drinkers.
We defined physical activity status based on respondents’ responses to questions about the frequency and duration of at least 10 min of vigorous-intensity or light-to-moderate-intensity activities during their leisure time. If respondents reported engaging in no physical activity, they were classified as physically inactive, if they reported >0 but <150 min/week of light-to-moderate-intensity physical activity and <75 min/week of vigorous-intensity physical activity or an equivalent combination of these two, they were classified as being insufficiently active. Physically active persons had ≥150 min/week or ≥75 min/week of light-to-moderate-intensity and vigorous-intensity physical activity. During data collection, the 2008 adult physical activity guidelines were applicable. When respondents reported moderate-intensity and vigorous-intensity physical activity, vigorous-intensity activity in minutes accounted for twice the estimate of minutes of moderate-intensity physical activity.47
Statistical analysis
Using the NCHS guidelines for analyzing NHIS data and taking the complex survey design into consideration, we pooled the 2 years of data, merging the Sample Adult and Person-Level files and applying sample weights to increase the accuracy of our estimates and obtain nationally representative estimates. The inferences obtained reflect the average for the target population over this period. Women who reported a prior pregnancy and whose region of birth were ‘elsewhere’ or ‘unknown’ or had missing information on GDM history (n=80) were excluded from the analysis.
We examined cardiometabolic risk profiles and the percentage with GDM history between US-born and foreign-born women using survey-weighted χ2 for categorical variables and t-tests for continuous variables. We used logistic regression to examine predictive probabilities of GDM by nativity status, using US-born women as a reference. Predictive margins were used to obtain the adjusted predictions and marginal effects for the models. The estimates from these predictive margins are a form of standardization that allows an inference to be drawn to the source population.48 Model 1 was unadjusted. Model 2 was age-adjusted (using the age at survey). Model 3 was further adjusted for income, education, insurance, smoking, overweight/obesity, physical activity status, and hypertension.
Using the 2010 US population as the standard with estimates for the following age groups: 18–25, 25–34, 35–44, 45–54, 55–64, 65–74, and ≥75 years,49 we also examined the age-standardized percentage with GDM history by nativity and duration of US residence. Finally, we examined the percentage with GDM history by race, ethnicity, and nativity status.
To explore the influence of duration of US residence on the GDM history among foreign-born women, we stratified foreign-born women by duration of US residence (<10 years vs ≥10 years). We then compared the sociodemographic and cardiometabolic risk profiles and the percentage with GDM history, among foreign-born women (<10 years and ≥10 years) using US-born women as reference. We performed sensitivity analysis with duration of US residence stratified as <15 years and ≥15 years. We used a two-sided alpha (α) level of ≤0.05 to determine statistical significance of results. All analyses were performed with Stata V.16.1 SE (StataCorp, College Station, Texas, USA).
Results
Sociodemographic characteristics and cardiometabolic risk profiles
The study sample of women (n=9525) who reported ever being pregnant and responded to the question about GDM had a mean age (±SD) of 36.5 (±0.1) years at survey. US-born women had a mean age of 36.3 (±0.1) years and were on average 1 year younger than the foreign-born women at the time of the survey (table 1). There were significant differences in sociodemographic factors between US-born and foreign-born women. While majority of the US-born women were NH whites (67.8%), followed by NH blacks (18.4%), Hispanics constituted most of the foreign-born group (55.3%), followed by NH Asians (21.3%) and NH whites (13.8%). Compared with foreign-born women, US-born women were more likely to be insured (89.8% vs 74.8%; p<0.001), employed (77.8% vs 65.6%; p<0.001), have a PIR of ≥2 (60.5% vs 49.5%; p<0.001), and have a usual place to go to when sick (88.6% vs 81.5%; p<0.001). Foreign-born women were more likely to be married (65.8% vs 51.3%; p<0.001) and have a bachelor’s degree or higher (33.4% vs 33.1%; p<0.001) compared with US-born women.
Sociodemographic characteristics of women participants by nativity status and length of stay (n=9525)
There were also differences in the cardiometabolic risk profiles between US-born and foreign-born women. US-born women were more likely to have a history of hypertension (18.3% vs 10.2%; p<0.001) compared with foreign-born women. The prevalence of current smoking (21.4% vs 4.4%; p<0.001), current light alcohol drinking (57.1% vs 40.3%; p<0.001), and current heavy alcohol drinking (16.8% vs 4.9%; p<0.001) was also higher among US-born compared with foreign-born women. A greater proportion of US-born women were more likely to have sufficient physical activity compared with foreign-born women (53.6% vs 45.8%; p<0.001). There was no difference in the prevalence of overweight/obesity between the two groups.
When we stratified the foreign-born women by duration of US residence, women with duration of residence ≥10 years were more likely to be employed, have a usual place to go to when sick and have sufficient physical activity (all p values <0.001) compared with those with <10 years of US residence. They also had a higher prevalence of hypertension, current light alcohol drinking, current heavy alcohol drinking, and current smoking (compared with foreign-born women with <10 years duration of US residence (table 1).
Crude and adjusted associations of gestational diabetes mellitus among nativity status
The percentage with a GDM history in the study sample was 10%, and it was higher among foreign-born women than US-born women (11.7% vs 9.6%). The age-standardized percentage GDM among foreign-born and US-born women was 10.2% and 9.2%, respectively.
Foreign-born women had 32% higher odds of GDM than US-born women after adjusting for age, income, education, insurance, smoking status, overweight/obesity, physical activity status, and hypertension (OR 1.32; 95% CI 1.09 to 1.60) (table 2).
Crude and adjusted OR and 95% CIs of GDM history among US-born and foreign-born persons
GDM and duration of US residence
Longer duration of US residence (≥10 years) was also associated with higher odds of GDM history among the foreign-born women. The age-standardized percentage with GDM history among foreign-born women with duration of residence ≥10 years and foreign-born women with duration of residence <10 years were 11.0% and 6.7%, respectively, compared with 9.2% in US-born women (table 3). In the fully adjusted model, the odds of GDM in foreign-born women with duration of US residence <10 years was not significantly different than that of US-born women (OR 0.94 95% CI 0.64 to 1.38). Foreign-born women with ≥10 years duration of US residence on the other hand had significantly higher odds of GDM compared with US-born women (OR 1.43 95% CI 1.17 to 1.76) (table 3).
Crude and adjusted OR and 95% CIs of GDM history by duration of stay
We additionally ran a sensitivity analysis to evaluate the impact of duration of US residence <15 years and ≥15 years and found similar results (online supplemental table A).
Supplemental material
In an exploratory analysis, we also evaluated the nativity-related disparities in GDM history by race and ethnicity (figure 2). We found that significantly higher percentage with GDM history among foreign-born women compared with their US-born counterparts was only observed among NH white and NH Asian women.

{kind=link}
{kind=link}
Age-standardized gestational diabetes mellitus history percentages among racial/ethnic groups by nativity status.
Discussion
In this nationally representative sample of women in the USA with pregnancy history, we found that the reported GDM history was higher among foreign-born women compared with US-born women. When we considered the duration of US residence, foreign-born women with shorter duration of US residence (<10 years) had lower odds of GDM history than US-born women—however the fully adjusted model that included cardiometabolic risk profile factors showed no significant difference in the odds of GDM history. In contrast, foreign-born women with longer duration of US residence (≥10 years) had higher odds of GDM history than US-born women. We also noted a higher prevalence of hypertension, smoking and alcohol use among foreign-born women with longer duration (10 years) of residence. The higher odds of GDM history among foreign-born women with longer duration of US residence (≥10 years) remained significant after adjusting for cardiometabolic risk factors, suggesting that other unmeasured confounders (eg, stress, discrimination, etc) may additionally contribute to the higher odds of GDM.
Our results are consistent with numerous studies which have found an increased risk of GDM among foreign-born women;14 15 19 20 22 25 as well as among some non-US-based studies, showing a positive relationship between duration of residence in the receiving country and GDM prevalence. In a Norwegian study (n=1 309 846), the prevalence of GDM increased with longer duration of residence in Norway, but with some heterogeneity by country of origin.50 Similarly, in a large Danish cohort study (n=725 482) of women, Kragelund Nieslen et al showed a positive association between longer duration of residence and GDM prevalence.51
These findings of a positive relationship between duration of residence in the USA and other high-income countries may be explained by the ‘Fetal Origins of Adult Disease’ hypothesis, which posits that malnutrition in utero, along with subsequent low birth weight, may lead to adaptations that affect beta-cell function and promote future insulin resistance.20 52 When the extrauterine environment matches the intrauterine environment (eg, low access to nutrients), such as what would be expected in under-resourced countries, this adaptation may be protective. However, when there is a mismatch in the intrauterine and extrauterine environment, such as what might occur when foreign-born women from under-resourced countries immigrate to the USA and are exposed to calorie dense westernized diets, these previously protective adaptations can become maladaptive, leading to insulin resistance and the development of other chronic diseases. Prior studies have shown a positive association between women who themselves had low birth weight newborns and their future risk of GDM.53 54 Additionally, a recent systematic review and meta-analysis confirmed that a westernized diet and in particular consumption of red meat and fast food, significantly increased GDM risk.55 Importantly, migration patterns, and in particular reason for migration may have important implications for this mismatch hypothesis—which assumes that immigrants are leaving more deprived and underdeveloped settings to enter the USA; when in fact, reasons for immigration vary widely (ie, to escape political turmoil, famine, and drought as in Ethiopian immigrants entering the USA in the 1980s, or because a country is experiencing surplus—as in Nigerian immigrants entering the USA because of government sponsorships during the oil boom of the 1970s)56 and may not always result in a mismatch of environments. Future studies should carefully consider migration patterns in their assessment of acculturation and its impact on health outcomes.
Since the health behaviors and sociocultural context of foreign-born women appear protective for other adverse pregnancy outcomes (eg, pre-eclampsia, low birth and preterm birth)16 57 and chronic conditions,44 there is ongoing interest in understanding why GDM is unique in terms of associations with nativity. The results of our investigation around duration of US residence within the context of cardiometabolic risk profile factors are unique and provide more nuance to this well-known association.
Since foreign-born women with shorter duration of US residence had lower prevalence of cardiometabolic risk factors than US-born women, our results highlight that unhealthy assimilation—the term used to describe the adoption of attributes of the host country that may be detrimental to health—may occur with longer duration of US residence and may contribute to incidence of cardiometabolic risk along with other factors.
Even though we were underpowered to fully examine the variation in nativity-associated outcomes by specific race and ethnicity groups, the pattern suggests that there is heterogeneity in the odds of GDM history among racial and ethnic groups. This is consistent with prior literature which has found significant heterogeneity both between and within racial/ethnic groups, and by country of origin.20 50 51 58 Importantly, this heterogeneity may have implications for understanding nativity-related disparities in GDM. For example, traditional risk factors for GDM, such as obesity, may also differ between foreign-born and US-born women. In a population-based study of 565 839 women in New York City, Janevic et al explored the influence of obesity on GDM risk among foreign-born and US-born women. The investigators found that obesity had a smaller influence on GDM risk for foreign-born women compared with US-born women.22 This result was consistent for all groups except for Asian and Indian (South Asian) women. Larger stratified analysis with more precise information on country of origin, migration timing and patterns, and other measures of acculturation are needed to better understand these nuances.
Clinical implications
These findings underscore that foreign-born women with longer duration of residence in the USA may be at greater risk for GDM than US-born women or foreign-born women with shorter residence in the USA. In terms of clinical management this has several potential implications. For example, while we were unable to examine diet and nutrition in this study, diet and nutrition are a large component of prevention and management in GDM; therefore, it may also be prudent to consider dietary patterns, which are heavily influenced by nativity, culture, and religious practices (eg, caloric/carbohydrate density of staple food sources, religious patterns of fasting). Additionally, healthy lifestyle choices are often mediated by socioeconomic status which is influenced by employment opportunities—and may be challenging or unstable as one establishes new residence in a country outside of their country of origin.
Nutrition recommendations should be attentive to dietary customs of foreign-born women, promote healthy diets that acknowledge the importance of such customs, with emphasis on the potential drawbacks of highly processed, calorie-dense westernized foods. Other considerations such as preferred language, health literacy, and other social determinants of health should also be considered to improve shared decision-making and adherence to healthy lifestyle promoting behaviors. Attention to these issues may help improve GDM-related outcomes among foreign-born women, who make up an increasing percentage of the US population.59
Limitations
The results of our study should be considered in light of several limitations. First, the cross-sectional nature of this study limits the ability to make causal inferences regarding the association between nativity and duration of residence in the USA and GDM as well as the timing of GDM diagnosis. Second, we did not have information on age at pregnancy and prior GDM history which are strong risk factors for GDM.60 61 The lack of information on age at pregnancy or GDM diagnosis in NHIS also limits the ability to establish temporality of our exposure and outcome. However, by restricting our sample to women of reproductive age, we are more likely to capture participants who had their reproductive years and thus a pregnancy with the outcome of interest in the USA. This reduces potential error in the estimate of the association between duration of US residence and GDM. Nevertheless, it is possible that some foreign-born participants had the outcome of interest in their country of origin, and since it has been reported that there is wide variation in screening recommendation and diagnostic criteria for GDM in low-income and middle-income countries,62 63 it is possible that the prevalence of GDM may be underestimated in this group. Third, the cardiometabolic risk profile factors examined were assessed at the time of the survey and may not reflect those that were proximal to pregnancy. Fourth, foreign-born women are not a homogenous group and have different cultural practices encompassing nutrition and social support. However, we were underpowered to stratify immigrants by region of origin and unable to evaluate these cultural factors. Finally, although we measured acculturation using the proxy of duration of US residence, acculturation is complex—its impact on health may be positive, negative, or neutral depending on the degree of assimilation, which we did not evalute.38 We were also unable to evaluate the impact of racial discrimination, which may adversely impact immigrant health.30 31
Despite these limitations, our study also has strengths. We used a nationally representative sample to provide contemporary estimates of the prevalence of GDM, we were able to evaluate health behaviors and we identified challenges and gaps that can be addressed in future studies. In particular, future GDM and nativity-related disparities in birth outcomes research should assess risk factors among large and diverse groups, with carefully documented social, environmental, and dietary patterns, as well as the evolving role of racial discrimination that may be unique to US contexts.
Conclusion
Greater duration of US residence may contribute to nativity-related disparities in women with GDM. Acculturation, including changing health-related behaviors, may have an important impact on maternal health outcomes of foreign-born women and should be further investigated to appropriately target interventions to reduce GDM and future cardiometabolic diseases.
Data availability statement
Data are available in a public, open access repository. The data used in this study are publicly available from the National Health Interview Survey (NHIS) website (https://www.cdc.gov/nchs/nhis/data-questionnaires-documentation.htm)
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @dcrchellemd, @rantocran, @Ellen_A_Boakye, @Wendy_LBennett, @GarimaVSharmaMD, @LisaCooperMD, @ycommodore
Contributors SMO, R-ANT-O, EB, and YC-M contributed to the design of the manuscript. SMO, R-ANT-O, and EB contributed to the analysis of the data. SMO, R-ANT-O, EB, YC-M, AAC, XW, GS, LAC, and YC-M made key intellectual contributions and contributed to the writing of the manuscript. SMO is the guarantor of this work and as such had access to the data, controlled the decision to publish, and accepts full responsibility for the finished work and the conduct of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.