
Abstract
Background:
The risks for several cancer types are increased in people with diabetes. Hyperglycaemia, hyperinsulinaemia, inflammation and altered hormonal concentrations are common characteristics between the two diseases and can all be linked to hyperglycaemia.
Methods:
Here, we use glycated haemoglobin (HbA1c) as a biomarker for chronic hyperglycaemia. We explore whether cancer risk increases with HbA1c, independent of diabetes, and, therefore, if risk is already increased below the diabetic HbA1c range, by analysing data from current studies linking HbA1c to risk of several cancer types.
Results:
The data reveal that chronic hyperglycaemia correlates with increased cancer risk for a number of cancers, except prostate cancer. Evidence is also provided that risk is already increased in the pre-diabetic and normal ranges for several cancers.
Conclusions:
These results merit urgent investigation into the risks and advantages of updating recommendations for stricter glycaemic control in diabetic and non-diabetic subjects, as this could help reduce the risk of cancer incidence and mortality.
Similar content being viewed by others

Main
People with established diabetes have an increased risk of developing certain cancer types compared with non-diabetics; the strongest associations are seen for endometrial, liver and pancreatic cancer, followed by kidney, oesophageal, colorectal, breast and bladder cancer, and leukaemia (Giovannucci et al, 2010; Habib and Rojna, 2013). It is, however, not clear whether hyperglycaemia, a hallmark of diabetes, correlates with increased cancer risk independent of diabetes. If such an association exists, then the cancer risk in persons with glucose levels lower than that required to diagnose diabetes might already be increased. This would have important diagnostic and therapeutic ramifications, which we investigate here.
Research surrounding the increasing prevalence of cancer and diabetes (Mathers and Loncar, 2006; Giovannucci et al, 2010; World Health Organization, 2010; Wagner and Brath, 2012) has established direct pathogenetic commonalities between these two chronic diseases. These include hyperinsulinaemia, hyperglycaemia, inflammation and altered concentrations of endogenous hormones.
The association of most cancers and diabetes with chronic inflammation (Pollak, 2012; Coussens et al, 2013) and the direct link between increased inflammatory signalling and high blood glucose levels in cancer models (Habib and Rojna, 2013) support the possibility that chronic hyperglycaemia may have a pivotal role in cancer risk in humans. Increased production of endogenous hormones can also be indirectly linked to hyperglycaemia via hyperinsulinaemia and obesity, and, therefore, also to diabetes and cancer risk (Montaruli et al, 2012; Patterson et al, 2013; Robien et al, 2013). Chronic hyperglycaemia in diabetes patients seems to be directly linked with the ubiquitous reliance of most cancer cells on high glucose flux (Hanahan and Weinberg, 2011; Mathews and Liebenberg, 2013). Onodera et al (2014) found that an increase in glucose uptake can activate oncogenic pathways in breast cells. This could potentially provide another pathway by which hyperglycaemia increases cancer incidence risk.
Chronic hyperglycaemia may be evaluated by measuring glycated haemoglobin (HbA1c) (American Diabetes Association, 2013), a biomarker of the average blood glucose concentration for a prolonged period of time (Travier et al, 2007; Habib and Rojna, 2013). Importantly, HbA1c may also be a good indicator of metabolic processes influencing levels of insulin (Saydah et al, 2003) or insulin-like growth factors, important for cancer pathogenesis (Habib and Rojna, 2013).
Most studies focus on the association between cancer risk and diabetes. This approach, however, does not provide evidence for the potential causal links between the two diseases (Giovannucci et al, 2010).
One study (Pisani, 2008) performed a meta-analysis on epidemiological studies linking hyperglycaemia and risk for colorectal and pancreatic cancers. The researcher only assessed risk in the highest compared with the lowest categories of exposure. Another study (Johnson and Bowker, 2011) performed a meta-analysis on the impact of glycaemic control in type 2 diabetic patients and found no decrease in cancer risk with increased glycaemic control. This meta-analysis may have been influenced by confounding factors such as insulin usage, which could increase cancer risk (Pollak, 2012). Habib and Rojna (2013) reviewed some of the most important studies on the association between cancer risk and hyperglycaemia. They, however, did not attempt to consolidate the evidence per cancer type or provide a dose–response relation.
No meta-analysis has yet been published that consolidates risk of different types of cancers with different HbA1c ranges, including glycaemic levels lower than that associated with diabetes. If cancer risk is lower at low HbA1c levels, then the incidence of cancer in the diabetic and non-diabetic populations could potentially be lowered by decreasing glucose levels. This could be achieved by means of appropriate lifestyle or therapeutic interventions, and by imposing stricter recommendations for glycaemic control.
Here, we perform dose–response meta-analyses on the current published evidence regarding HbA1c levels and risk of various cancers. This post hoc analysis attempts to establish whether cancer risk is already elevated in normal and pre-diabetic HbA1c ranges. The overall goal is to determine whether HbA1c concentrations can effectively quantify cancer risk independent of diabetes.
Materials and methods
Study selection
Only English-language articles were included. Studies from 1960 to the present (date last searched – 9 January 2014) were included in the search. Articles using the following risk measures were included: relative risk (RR), odds ratio (OR) or hazard ratio (HR). For studies to be included in the quantitative meta-analysis, they had to provide risk data for at least three HbA1c levels. Literature searches were performed using Science Direct and Scopus to identify articles that relate HbA1c to the risk of cancer incidence (primary or recurrence) or mortality. More articles were identified from the reference lists of surveyed articles.
Search terms included a number of MeSH terms and were combinations of the following: (‘cancer’ OR ‘malignancy’ OR ‘tumor’ OR ‘tumour’ OR ‘neoplasm’ OR ‘neoplasia’) AND (‘hemoglobin a1c’ OR ‘hba1c’ OR ‘glycated hemoglobin’ OR ‘glycosylated hemoglobin’ OR ‘a1c’ OR ‘haemoglobin a1c’ OR ‘glycated haemoglobin’ OR ‘glycosylated haemoglobin’ OR ‘glycohemoglobin a’ OR ‘glycohaemoglobin a’) in the title of the study.
The trends adjusted for the most confounding variables were used, where sufficient information was available on that trend. This was done so that the effects of most of the potential confounders could be adjusted for. This may, however, have increased the heterogeneity between studies, as not all studies adjusted for the same confounders. Only studies providing data on specific cancer types were included (not studies referring to cancer in general).
It was assumed that all studies used the National Glycohemoglobin Standardization Program (NGSP) HbA1c reference, unless explicitly stated otherwise in a specific study. Suitable conversion to the NGSP reference was performed for three studies (Stocks et al, 2007, 2008; Cust et al, 2009) that used the Swedish monoS standard, using the relation NGSP (%)=(monoS+0.8925)/0.9718. Using the NGSP reference, ‘diabetes’ is deemed to exist at HbA1c levels greater than 6.5% (American Diabetes Association, 2013); ‘pre-diabetes’ if HbA1c levels are between 5.7% and 6.4% (American Diabetes Association, 2013). The ‘normal glycaemic’ range is taken to span from ∼4–5.7% (American Diabetes Association, 2013).
Data extraction
The following data were extracted from the studies: reference details, number of cases per HbA1c level for OR, RR and HR, number of controls per HbA1c level for OR, total number of persons per HbA1c level for RR, number of person-years per HbA1c level for HR, gender, cancer site, whether the risk was measured in RR, OR or HR, the risk per HbA1c range, HbA1c range or level and the 95% confidence intervals (CIs) per HbA1c level. Additional information was obtained from the authors of two studies to be able to include these studies in the quantitative analysis.
Statistical analyses
When a range of HbA1c values was provided, a single value was chosen per HbA1c category using method 1 in Hartemink et al (2006). It is acknowledged that the method that is used to select a single value per dose–response category could potentially affect the outcome (Hartemink et al, 2006). The method works as follows. Where a range was specified for a dose, the midpoint of the range was selected as the point representing that range; where an open-ended range was specified, the dose for the lower open-ended range was calculated by subtracting half of the width of the second lowest range from the lowest value specified (the top value of the bottom open-ended range) (Hartemink et al, 2006); the dose for the upper open-ended range was calculated by adding the width of the second highest range to the highest value specified (bottom value of the upper open-ended range) (Hartemink et al, 2006).
Dose–response meta-analyses were performed per cancer type and for cancer incidence and mortality separately using the dosresmeta R package (Crippa, 2013; R Core Team, 2013). This is the R-equivalent of the GLST Stata-module developed by Orsini et al (2006, 2012).
Risk estimates were transformed using the natural logarithm (ln). The reference HbA1c level per study was subtracted from each HbA1c level in the study, resulting in a model fitted through the origin (i.e., no intercept).
Linear and restricted cubic spline (RCS) models (with three knots, located at the 10th, 50th and 90th percentiles of the data) of the natural logarithm-transformed risk estimates were developed using random-effects meta-analysis methods, to incorporate heterogeneity. If, for a certain cancer type, only a single study was available, and that study had fewer than six exposure levels, only a linear model was fitted, as the function that develops the RCS models requires at least six data points. The graphical displays of the statistically significant models obtained during the analyses were referenced to the lowest HbA1c level for all the studies included in a model.
To assess non-linearity, the null hypothesis that the coefficient of the second spline is zero was tested. A significance level of P<0.05 was used.
Lack of goodness of fit and heterogeneity was determined by assessing whether the P-value from the chi-squared test was smaller than 0.1. I2 values were determined for each model.
Combined and separate models for RR, OR and HR were developed to assess whether the risk measure, and in effect the type of study, could influence the results.
Results
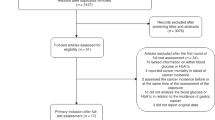
The study selection process is illustrated in Figure 1. Thirty-six studies were identified through database searching. Thirty-two studies were identified from the reference lists of surveyed articles. Two duplicate studies were removed. The remaining 66 records were screened. Ten articles were not relevant to the study aims (e.g., they did not address cancer). For six of the records, full-text articles were not available or referred to conference abstracts. Fifty full-text articles were assessed. Of these, 18 articles were excluded as they either did not provide data on a specific cancer type (9 studies), they did not provide data on cancer (2 studies) or they used glycaemic measures other than HbA1c (7 studies). Thirty-two studies remained that were relevant for the qualitative synthesis. Eighteen studies were excluded from the quantitative analysis as they did not provide information on cancer incidence or mortality, but rather on stage or grade of cancer (4 studies), they provided information on cancer pre-cursors, such as adenoma, adenomatous polyps or benign neoplasia (5 studies), they did not provide data on RR, OR or HR (2 studies), they specified fewer than three HbA1c ranges (4 studies), the study population was already included in another study (2 studies) or enough information on the number of cases or person-years per HbA1c level was not available (1 study). Fourteen studies remained that were included in the quantitative meta-analyses. Of these, thirteen studies provided data on cancer incidence only, while one study provided data on cancer incidence as well as mortality (Joshu et al, 2012).

Flow diagram showing the study selection process ( Moher et al, 2009).
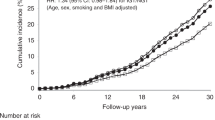
The statistically significant or border-line significant models that were obtained during the dose–response analyses are shown in Figures 2, 3, 4, 5, 6, 7, 8. The plots are referenced to the lowest HbA1c level in the studies included in each model.

Relationship between risk for breast cancer incidence and HbA1c.

Relationship between risk for colorectal cancer incidence and HbA1c.

Relationship between risk for colorectal cancer mortality and HbA1c.

Relationship between risk for gastric cancer incidence and HbA1c.

Relationship between risk for pancreatic cancer incidence and HbA1c.

Relationship between risk for prostate cancer incidence and HbA1c.

Relationship between risk for respiratory cancer incidence (including lung cancer) and HbA1c.
Female genital cancer
Quantitative analysis
Two studies (Travier et al, 2007; Miao Jonasson et al, 2012) on female genital cancer incidence were included in the quantitative analysis. Both used the HR as a risk measure. No statistically significant models were obtained in the analysis (P=0.2961 for increasing log-linear model, Pnon-linearity=0.3274 for increasing-decreasing RCS model).
Qualitative analysis
Travier et al (2007) found a statistically significant (HR=2.84, 95% CI=1.35–5.98) increased risk in the 6% to 7% HbA1c range, compared with the reference risk in the <6% range. The risk was also increased in the >7% range, but not significantly (HR=2.01, 95% CI=0.69–5.89). Miao Jonasson et al (2012) found no statistically significant associations for cancer risk in the baseline (slightly decreased HRs) or updated mean (slightly increased HRs) HbA1c groups for a group of people with type 2 diabetes. Levran et al (1984) revealed an increased number of endometrial cancer cases with HbA1c above 6.5%, as compared with below 6.5%. The distribution of controls was more even across all of the HbA1c ranges. They, however, did not provide risk measures for comparison. Levitan et al (2008) found no statistically significant trend (P=0.53) for uterine or ovarian cancer mortality risk. Stevens et al (2012) found some evidence of increased endometrial cancer stage with increasing HbA1c, but this was not statistically significant (P=0.07).
Liver cancer
Quantitative analysis
One study (Travier et al, 2007) was included in the quantitative analysis for liver cancer incidence. The increasing log-linear HR model obtained from this study was not statistically significant (P=0.5737).
Qualitative analysis
Two studies that were excluded from the quantitative analysis as they did not provide enough HbA1c levels (Donadon et al, 2010; Kaneda et al, 2012) found changes in hepatocellular carcinoma (HCC) risk as HbA1c increased. Kaneda et al (2012) found a large risk (HR=3.551, P=0.03) for HCC recurrence as the HbA1c level increased above 6.5% for patients with diabetes. Donadon et al (2010) found that the OR for HCC increased by 1.508 for each percentage increase in HbA1c for type 2 diabetic patients compared with controls with liver cirrhosis (P=0.0005). Compared with the normal control group, the OR increased by 1.265 per 1% increase in HbA1c – this was, however, not statistically significant (P=0.1172).
Pancreatic cancer
Quantitative analysis
One study (Grote et al, 2011) was included in the quantitative analysis. The OR increasing log-linear model, including diabetic participants, was statistically significant (P=0.0049). The increasing log-linear model, excluding diabetic participants, was also statistically significant (P=0.0148).
Qualitative analysis
Another study (Levitan et al, 2008) found no statistically significant trends for pancreatic cancer mortality (P=0.40), with decreased risk (RR=0.86) in the lower normal HbA1c range of 4.88–5.08% and increased risk (RR=1.36) in the upper normal range (5.09–5.59%), compared with the reference group (2.27–4.87%).
Prostate cancer
Quantitative analysis
Four studies were included in the quantitative analysis for prostate cancer incidence (Stocks et al, 2007; Travier et al, 2007; Joshu et al, 2012; Miao Jonasson et al, 2012), while only one study (Joshu et al, 2012) was included in the analysis for mortality. The OR decreasing log-linear model obtained from the Stocks et al (2007) study was border-line statistically significant (P=0.0596), while none of the other models were statistically significant (P=0.1114 for the decreasing combined log-linear model, P=0.1783 for the decreasing HR log-linear model, P=0.6502 for the decreasing HR mortality log-linear model).
Qualitative analysis
Rusu et al (2011) found that HbA1c was statistically significantly (P=0.0001) lower in patients with prostate cancer (HbA1c=6%) than in those without cancer (HbA1c=7.1%) or in patients with benign prostatic hyperplasia (HbA1c=7.4%). No adjustments were made for confounders in this study.
Kim et al (2010a) revealed statistically significant (P=0.001) increased risks for higher pathological Gleason score cancer with increasing HbA1c level in a population of diabetic men. Hong et al (2009) found a significantly higher rate of high pathological Gleason score cancers (P=0.005) and extraprostatic extension (P=0.043) in diabetic men with HbA1c levels ⩾6.5% than in those with HbA1c levels lower than 6.5%.
Colorectal cancer
Quantitative analysis
Nine studies presented data on colorectal cancer incidence. Two of these studies (Platz et al, 1999; Khaw et al, 2004) were excluded from the quantitative analysis as they provided data from the same cohorts as other studies already included. Seven studies remained that were included in the quantitative analysis (HR – Joshu et al, 2012; RR – Lin et al, 2005; OR – Rinaldi et al, 2008; OR – Saydah et al, 2003; OR – Stocks et al, 2008; HR – Travier et al, 2007; OR – Wei et al, 2005). One study also presented data on colorectal cancer mortality (HR – Joshu et al, 2012). The colorectal cancer incidence combined RCS model (Pnon-linearity=0.0068, Pheterogeneity=0.2046, I2=21.4%) and HR RCS model (Pnon-linearity=0.0261, Pheterogeneity=0.8494, I2=1%) both showed a decreased risk at lower HbA1c levels followed by an increased risk at higher HbA1c levels. The combined log-linear model (P=0.0325, Pheterogeneity=0.1526, I2=33.2%) and OR log-linear model (P=0.0072, Pheterogeneity=0.2945, I2=18.9%) both showed statistically significant increasing trends. The mortality RCS HR model was also statistically significant (Pnon-linearity=0.0180, Pheterogeneity=0.9849, I2=1%), with decreasing risk at lower HbA1c levels, and increasing risk at higher HbA1c levels. The other models were not statistically significant (P=0.3089 for increasing HR log-linear model, P=0.1486 for OR RCS decreasing-increasing model, P=0.3942 for decreasing RR log-linear model).
Qualitative analysis
Further to the results from the dose–response relation, Khaw et al (2004) found a significantly increased risk as HbA1c increased in the combined (P<0.001), men-only group (P<0.001) and women-only group (P=0.03). The risk in the women-only group was decreased in the 5–5.9% range (RR=0.7), but increased above this range. Continuous analysis per 1% increase in HbA1c revealed an increase of RR=1.30 for the combined group (P=0.02), RR=1.35 for the men-only group (P=0.02) and RR=1.20 for the women-only group (P=0.26). The authors found that the increased risk for colorectal cancer in diabetic patients was largely due to the increase in HbA1c and not due to diabetes status. Platz et al (1999) and Siddiqui et al (2008a) found a significant increase in risk for advanced-stage colorectal cancer with higher HbA1clevels (P=0.02 and P=0.002, respectively).
The risks for colorectal cancer pre-cursors (adenomatous and/or advanced adenomatous polyps) were significantly increased with increasing HbA1c levels in diabetic and non-diabetic subjects (Siddiqui et al, 2008b; Kim et al, 2010b). Hsu et al (2012) found an increase of OR=1.25 in colorectal neoplasia for each percentage increase in HbA1c level for men and women (P=0.02). HbA1c was not statistically significantly associated with colorectal adenoma, distal colorectal adenoma or advanced adenoma in two studies (Wei et al, 2006; Yang et al, 2010).
Breast cancer
Quantitative analysis
Six studies on breast cancer incidence (HR – Joshu et al, 2012; HR – Miao Jonasson et al, 2012; HR – Travier et al, 2007; HR – Erickson et al, 2011; OR – Cust et al, 2009; RR – Lin et al, 2006) and one study on cancer mortality (HR – Joshu et al, 2012) were included in the quantitative analysis. A statistically significant RCS model for combined risk (Pnon-linearity=0.0260, Pheterogeneity=0.6457, I2=1%), which showed decreased risk at lower HbA1c levels and increased risk at higher HbA1c levels, as well as a border-line statistically significant increasing log-linear model for HR (P=0.0783, Pheterogeneity=0.6948, I2=1%) was obtained. The other models were all statistically non-significant (P=0.2329 for increasing combined log-linear model, Pnon-linearity=0.3118 for HR decreasing-increasing RCS model, P=0.2323 for decreasing OR log-linear model, Pnon-linearity=0.2844 for increasing-decreasing RCS model, P=0.2007 for decreasing RR log-linear model, P=0.1789 for increasing HR log-linear mortality model).
Qualitative analysis
Two studies did not adjust for confounders and found contrasting results. Yadav et al (2012) observed that HbA1c increased in pre- and post-menopausal breast cancer cases. Contrarily, Nemesure et al (2009) found decreased HbA1c in pre- and post-menopausal breast cancer cases.
Levitan et al (2008) found no statistically significant linear trend for breast cancer mortality with increasing HbA1c level (P=0.23).
Gastric cancer
Quantitative analysis
Two studies on gastric (stomach) cancer incidence were included in the quantitative analysis (HR – Ikeda et al, 2009; HR – Travier et al, 2007). The increasing log-linear trend obtained from these studies was statistically significant (P=0.0171, Pheterogeneity=0.9439, I2=1%).
Qualitative analysis
No additional studies were available for discussion.
Respiratory cancer, including lung cancer
Quantitative analysis
Two studies on respiratory or lung cancer incidence were included in the quantitative analysis (HR – Joshu et al, 2012; HR – Travier et al, 2007). The RCS model obtained from these studies was statistically significant (Pnon-linearity=0.0353, Pheterogeneity=0.1537, I2=40.1%), with increasing risk at lower HbA1c levels, and decreasing risk at higher HbA1c levels. Neither the increasing log-linear HR mortality model (P=0.1573), nor the increasing-decreasing RCS HR mortality model from the Joshu et al (2012) study was statistically significant (Pnon-linearity=0.2996).
Qualitative analysis
The Levitan et al (2008) study found increasing lung cancer mortality risk with increased HbA1c level, but the linear trend was not statistically significant (P=0.22).
Other cancers
Quantitative analysis
Results from other cancer types investigated were not statistically significant. These cancer types included lymphoma and leukaemia (P=0.5427 for the decreasing log-linear model), as well as melanoma (P=0.5514 for the increasing log-linear model). One study (HR – Travier et al, 2007) presented results on each type of cancer.
Qualitative analysis
Levitan et al (2008) found an increase in RR for lymphoma or leukaemia mortality as HbA1c increased. This was, however, not statistically significant (P=0.18 for a linear trend).
Discussion
Quantitative analysis
Results from the dose–response meta-analysis revealed the following statistically significant or border-line significant results:
-
Increasing log-linear models for breast cancer (HR), colorectal cancer (OR and combined), gastric cancer (HR) and pancreatic cancer (OR).
-
Decreasing log-linear model for prostate cancer (OR).
-
Increased risk above 8.5% for breast cancer (combined) and colorectal cancer (HR for incidence and mortality), above 6.5% for colorectal cancer (combined) and increasing trend up to 7% and decreasing risk above 7% for respiratory cancer (HR).
The following relations were not statistically significant:
-
Increasing log-linear models for female genital cancer (HR), liver cancer (HR), colorectal cancer (HR), breast cancer (combined and HR mortality), respiratory (HR) and melanoma (HR).
-
Decreasing log-linear models for prostate cancer (combined, HR and HR mortality), colorectal (RR), breast (OR and RR) and lymphoma and leukaemia (HR).
Qualitative analysis
The qualitative analysis revealed some additional information. Cancer stage for female genital cancer was found to be non-significantly increased with increasing HbA1c. Liver cancer incidence increased significantly for diabetics and in patients with HbA1c above 6.5%. A significantly higher rate of high-grade prostatic tumours and extraprostatic extension was present with increasing HbA1c. For colorectal cancer, advanced stage colorectal cancer incidence and pre-cursor incidence increased with increasing HbA1c level. Respiratory/lung cancer, as well as lymphoma and leukaemia, mortality was non-significantly increased with increasing HbA1c level.
Conclusions
Our study corroborates that cancer sites should be investigated separately, as the observed trends differ between cancer sites. Evidence is provided that indicates:
-
Cancer incidence risk is already increased in the pre-diabetic and normal ranges for colorectal, gastric, pancreatic and respiratory cancers, although the results are not the same for all risk measures.
-
Cancer incidence is higher at HbA1c levels in the diabetic range for colorectal, gastric, pancreatic, breast and liver cancers.
There is possible evidence for:
-
Decreased risk of prostate cancer incidence with increasing HbA1c level, and already in the pre-diabetic and normal ranges.
-
Increased risk of breast cancer incidence in the diabetic, pre-diabetic and normal ranges.
Our study reveals that chronic hyperglycaemia, as quantified by HbA1c levels, correlates with increased cancer risk in colorectal, gastric, liver and pancreatic cancers, and possibly breast cancer, while correlating with decreased prostate cancer risk. The relations for other cancer types investigated are not statistically significant. It is also clear that there is increased risk for higher cancer stage/grade and cancer pre-cursor incidence for some cancer types with increasing HbA1c level.
The near-linear association of HbA1c levels with risk of several cancers supports the conjecture that it might be possible to use HbA1c as an independent metabolic biomarker for cancer risk in diabetic or non-diabetic persons. Significantly, the study also provides preliminary evidence for an already increased cancer risk in the normal and pre-diabetic categories for a number of cancers. The incidence of cancer in the diabetic and non-diabetic populations could, therefore, potentially be reduced by decreasing glucose levels. This could be achieved by means of appropriate lifestyle or therapeutic interventions, and by imposing stricter recommendations for glycaemic control (Krone and Ely, 2005).
The risks and advantages of updating recommendations for stricter glycaemic control (in diabetic and non-diabetic subjects) merit urgent investigation. Indications are that such stricter glycaemic control measures could help reduce the risk for cancer incidence and mortality (Krone and Ely, 2005) as long as care is taken to ensure that stricter glycaemic control does not result in hypoglycaemia, which may have other deleterious effects.
Change history
29 April 2014
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
American Diabetes Association (2013) Standards of medical care in diabetes - 2013. Diabetes Care 36 (Suppl 1): S11–S66.
Coussens LM, Zitvogel L, Palucka AK (2013) Neutralizing tumor-promoting chronic inflammation: a magic bullet. Science 339 (6117): 286–291.
Crippa A (2013) Dosresmeta: Performing dose-response meta-analysis, computer software, http://cran.r-project.org/web/packages/dosresmeta/index.html.
Cust AE, Stocks T, Lukanova A, Lundin E, Hallmans G, Kaaks R, Jonsson H, Stattin P (2009) The influence of overweight and insulin resistance on breast cancer risk and tumour stage at diagnosis: a prospective study. Breast Cancer Res Treat 113 (3): 567–576.
Donadon V, Balbi M, Valent F, Avogaro A (2010) Glycated hemoglobin and antidiabetic strategies as risk factors for hepatocellular carcinoma. World J Gastroenterol 16 (24): 3025–3032.
Erickson K, Patterson RE, Flatt SW, Natarajan L, Parker BA, Heath DD, Laughlin GA, Saquib N, Rock CL, Pierce JP (2011) Clinically defined type 2 diabetes mellitus and prognosis in early-stage breast cancer. J Clin Oncol 29 (1): 54–60.
Giovannucci E, Harlan DM, Archer MC, Bergenstal RM, Gapstur SM, Habel LA, Pollak M, Regensteiner JG, Yee D (2010) Diabetes and cancer: a consensus report. Diabetes Care 33 (7): 1674–1685.
Grote VA, Rohrmann S, Nieters A, Dossus L, Tjønneland A, Halkjær J, Overvad K, Fagherazzi G, Boutron-Ruault MC, Morois S, Teucher B, Becker S, Sluik D, Boeing H, Trichopoulou A, Lagiou P, Trichopoulos D, Palli D, Pala V, Tumino R, Vineis P, Panico S, Rodríguez L, Duell EJ, Molina-Montes E, Dorronsoro M, Huerta JM, Ardanaz E, Jeurnink SM, Beulens JW, Peeters PH, Sund M, Ye W, Lindkvist B, Johansen D, Khaw KT, Wareham N, Allen N, Crowe F, Jenab M, Romieu I, Michaud DS, Riboli E, Romaguera D, Bueno-de-Mesquita HB, Kaaks R (2011) Diabetes mellitus, glycated haemoglobin and C-peptide levels in relation to pancreatic cancer risk: a study within the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. Diabetologia 54 (12): 3037–3046.
Habib SL, Rojna M (2013) Diabetes and risk of cancer. ISRN Oncol 2013: 583786.
Hanahan D, Weinberg RA (2011) Hallmarks of cancer: the next generation. Cell 144 (5): 646–674.
Hartemink N, Boshuizen HC, Nagelkerke NJ, Jacobs MA, van Houwelingen HC (2006) Combining risk estimates from observational studies with different exposure cutpoints: a meta-analysis on body mass index and diabetes type 2. Am J Epidemiol 163 (11): 1042–1052.
Hong SK, Lee ST, Kim SS, Min KE, Byun SS, Cho SY, Choe G, Lee SE (2009) Significance of preoperative HbA1c level in patients with diabetes mellitus and clinically localized prostate cancer. Prostate 69 (8): 820–826.
Hsu YC, Chiu HM, Liou JM, Chang CC, Lin JT, Liu HH, Wu MS (2012) Glycated hemoglobin A1c is superior to fasting plasma glucose as an independent risk factor for colorectal neoplasia. Cancer Causes Control 23 (2): 321–328.
Ikeda F, Doi Y, Yonemoto K, Ninomiya T, Kubo M, Shikata K, Hata J, Tanizaki Y, Matsumoto T, Iida M, Kiyohara Y (2009) Hyperglycemia increases risk of gastric cancer posed by Helicobacter pylori infection: a population-based cohort study. Gastroenterology 136 (4): 1234–1241.
Johnson JA, Bowker SL (2011) Intensive glycaemic control and cancer risk in type 2 diabetes: a meta-analysis of major trials. Diabetologia 54 (1): 25–31.
Joshu CE, Prizment AE, Dluzniewski PJ, Menke A, Folsom AR, Coresh J, Yeh HC, Brancati FL, Platz EA, Selvin E (2012) Glycated hemoglobin and cancer incidence and mortality in the Atherosclerosis in Communities (ARIC) study, 1990–2006. Int J Cancer 131 (7): 1667–1677.
Kaneda K, Uenishi T, Takemura S, Shinkawa H, Urata Y, Sakae M, Yamamoto T, Kubo S (2012) The influence of postoperative glycemic control on recurrence after curative resection in diabetics with hepatitis C virus-related hepatocellular carcinoma. J Surg Oncol 105 (6): 606–611.
Khaw KT, Wareham N, Bingham S, Luben R, Welch A, Day N (2004) Preliminary communication: glycated hemoglobin, diabetes, and incident colorectal cancer in men and women: a prospective analysis from the European Prospective Investigation into Cancer - Norfolk Study. Cancer Epidemiol Biomarkers Prev 13 (6): 915–919.
Kim HS, Presti JC Jr, Aronson WJ, Terris MK, Kane CJ, Amling CL, Freedland SJ (2010a) Glycemic control and prostate cancer progression: results from the SEARCH database. Prostate 70 (14): 1540–1546.
Kim BJ, Kim YH, Sinn DH, Kang KJ, Kim JY, Chang DK, Son HJ, Rhee PL, Kim JJ, Rhee JC (2010b) Clinical usefulness of glycosylated hemoglobin as a predictor of adenomatous polyps in the colorectum of middle-aged males. Cancer Causes Control 21 (6): 939–944.
Krone CA, Ely JTA (2005) Controlling hyperglycemia as an adjunct to cancer therapy. Integr Cancer Ther 4 (1): 25–31.
Levitan EB, Liu S, Stampfer MJ, Cook NR, Rexrode KM, Ridker PM, Buring JE, Manson JE (2008) HbA1c measured in stored erythrocytes and mortality rate among middle-aged and older women. Diabetologia 51 (2): 267–275.
Levran D, Modan M, Menczer J, Dulitzy M (1984) Increased rate of glucose intolerance in endometrial cancer - a community-based study. Gynecol Obstet Invest 18 (4): 190–193.
Lin J, Ridker PM, Pradhan A, Lee IM, Manson JE, Cook NR, Buring JE, Zhang SM (2005) Hemoglobin A1c concentrations and risk of colorectal cancer in women. Cancer Epidemiol Biomarkers Prev 14 (12): 3010–3012.
Lin J, Ridker PM, Rifai N, Lee IM, Manson JE, Buring JE, Zhang SM (2006) A prospective study of hemoglobin A1c concentrations and risk of breast cancer in women. Cancer Res 66 (5): 2869–2875.
Mathers CD, Loncar D (2006) Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 3 (11): 2011–2030.
Mathews EH, Liebenberg L (2013) Short-term starvation for cancer control in humans. Exp Gerontol 48 (11): 1293.
Miao Jonasson J, Cederholm J, Eliasson B, Zethelius B, Eeg-Olofsson K, Gudbjörnsdottir S (2012) HbA1c and cancer risk in patients with type 2 diabetes – a nationwide population-based prospective cohort study in Sweden. PLoS One 7 (6): e38784.
Moher D, Liberati A, Tetzlaff J, Altman DG PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151 (4): 264–269.
Montaruli A, Patrini P, Roveda E, Carandente F (2012) Physical activity and breast cancer. Sport Sci Health 8 (1): 1–13.
Nemesure B, Wu SY, Hambleton IR, Leske MC, Hennis AJ Barbados National Cancer Study Group (2009) Risk factors for breast cancer in a black population - The Barbados National Cancer Study. Int J Cancer 124 (1): 174–179.
Onodera Y, Nam JM, Bissell MJ (2014) Increased sugar uptake promotes oncogenesis via EPAC/RAP1 and O-GlcNAc pathways. J Clin Invest 124 (1): 367–384.
Orsini N, Bellocco R, Greenland S (2006) Generalized least squares for trend estimation of summarized dose–response data. Stata J 6 (1): 40–57.
Orsini N, Li R, Wolk A, Khudyakov P, Spiegelman D (2012) Meta-analysis for linear and nonlinear dose-response relations: examples, an evaluation of approximations, and software. Am J Epidemiol 175 (1): 66–73.
Patterson RE, Rock CL, Kerr J, Natarajan L, Marshall SJ, Pakiz B, Cadmus-Bertram LA (2013) Metabolism and breast cancer risk: frontiers in research and practice. J Acad Nutr Diet 113 (2): 288–296.
Pisani P (2008) Hyper-insulinaemia and cancer, meta-analyses of epidemiological studies. Arch Physiol Biochem 114 (1): 63–70.
Platz EA, Hankinson SE, Rifai N, Colditz GA, Speizer FE, Giovannucci E (1999) Glycosylated hemoglobin and risk of colorectal cancer and adenoma (United States). Cancer Causes Control 10 (5): 379–386.
Pollak M (2012) The insulin and insulin-like growth factor receptor family in neoplasia: an update. Nat Rev Cancer 12 (3): 159–169.
R Core Team (2013) R: A language and environment for statistical computing, computer software, http://www.R-project.org/.
Rinaldi S, Rohrmann S, Jenab M, Biessy C, Sieri S, Palli D, Tumino R, Mattiello A, Vineis P, Nieters A, Linseisen J, Pischon T, Boeing H, Hallmans G, Palmqvist R, Manjer J, Wirfält E, Crowe FL, Khaw KT, Bingham S, Tjønneland A, Olsen A, Overvad K, Lund E, Skeie G, Clavel-Chapelon F, Boutron-Ruault MC, de Lauzon-Guillain B, Ardanaz E, Jakszyn P, Ramon Quiros J, Chirlaque MD, Sanchez MJ, Dorronsoro M, Trichopoulou A, Lagiou P, Trichopoulos D, Bueno-de-Mesquita HB, van Duijnhoven FJ, Peeters PH, Slimani N, Ferrari P, Byrnes GB, Riboli E, Kaaks R (2008) Glycosylated hemoglobin and risk of colorectal cancer in men and women, the European Prospective Investigation into Cancer and Nutrition. Cancer Epidemiol Biomarkers Prev 17 (11): 3108–3115.
Robien K, Rock CL, Demark-Wahnefried W (2013) Nutrition and cancers of the breast, endometrium, and ovary. In: Nutrition in the Prevention and Treatment of Disease, Coulston AM, Boushey CJ, Ferruzzi MG (eds) pp 657–672. Elsevier: London.
Rusu F, Rusu E, Radulian G, Enache G, Jinga M, Rusu A, Jinga V, Codreanu O, Mischianu D, Cheta D (2011) Screening for prostatic tumors in metabolic syndrome patients in Romania. Acta Endo 7 (1): 47–58.
Saydah SH, Platz EA, Rifai N, Pollak MN, Brancati FL, Helzlsouer KJ (2003) Association of markers of insulin and glucose control with subsequent colorectal cancer risk. Cancer Epidemiol Biomarkers Prev 12 (5): 412–418.
Siddiqui AA, Spechler SJ, Huerta S, Dredar S, Little BB, Cryer B (2008a) Elevated HbA1c is an independent predictor of aggressive clinical behavior in patients with colorectal cancer: a case-control study. Dig Dis Sci 53 (9): 2486–2494.
Siddiqui AA, Maddur H, Naik S, Cryer B (2008b) The association of elevated HbA1c on the behavior of adenomatous polyps in patients with type-II diabetes mellitus. Dig Dis Sci 53 (4): 1042–1047.
Stevens EE, Yu S, Van Sise M, Pradhan TS, Lee V, Pearl ML, Lee YC, Abulafia O (2012) Hemoglobin A1c and the relationship to stage and grade of endometrial cancer. Arch Gynecol Obstet 286 (6): 1507–1512.
Stocks T, Lukanova A, Johansson M, Rinaldi S, Palmqvist R, Hallmans G, Kaaks R, Stattin P (2008) Components of the metabolic syndrome and colorectal cancer risk: a prospective study. Int J Obes 32 (2): 304–314.
Stocks T, Lukanova A, Rinaldi S, Biessy C, Dossus L, Lindahl B, Hallmans G, Kaaks R, Stattin P (2007) Insulin resistance is inversely related to prostate cancer: a prospective study in Northern Sweden. Int J Cancer 120 (12): 2678–2686.
Travier N, Jeffreys M, Brewer N, Wright CS, Cunningham CW, Hornell J, Pearce N (2007) Association between glycosylated hemoglobin and cancer risk: a New Zealand linkage study. Ann Oncol 18 (8): 1414–1419.
Wagner KH, Brath H (2012) A global view on the development of non communicable diseases. Prev Med 54 (Suppl): S38–S41.
Wei EK, Ma J, Pollak MN, Rifai N, Fuchs CS, Hankinson SE, Giovannucci E (2005) A prospective study of C-peptide, insulin-like growth factor-I, insulin-like growth factor binding protein-1, and the risk of colorectal cancer in women. Cancer Epidemiol Biomarkers Prev 14 (4): 850–855.
Wei EK, Ma J, Pollak MN, Rifai N, Fuchs CS, Hankinson SE, Giovannucci E (2006) C-peptide, insulin-like growth factor binding protein-1, glycosylated hemoglobin, and the risk of distal colorectal adenoma in women. Cancer Epidemiol Biomarkers Prev 15 (4): 750–755.
World Health Organization (2010) Global Status Report on Noncommunicable Diseases 2010.
Yadav NK, Poudel B, Thanpari C, Chandra Koner B (2012) Assessment of biochemical profiles in premenopausal and postmenopausal women with breast cancer. Asian Pac J Cancer Prev 13 (7): 3385–3388.
Yang YX, Habel LA, Capra AM, Achacoso NS, Quesenberry CP Jr, Ferrara A, Levin TR, Lewis JD (2010) Serial glycosylated hemoglobin levels and risk of colorectal neoplasia among patients with type 2 diabetes mellitus. Cancer Epidemiol Biomarkers Prev 19 (12): 3027–3036.
Acknowledgements
This work was supported by TEMM International (Pty) Ltd. We would like to thank Professor Eugene Fine (Albert Einstein College of Medicine) for his valuable comments and suggestions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License.
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
de Beer, J., Liebenberg, L. Does cancer risk increase with HbA1c, independent of diabetes?. Br J Cancer 110, 2361–2368 (2014). https://doi.org/10.1038/bjc.2014.150
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2014.150
Keywords
This article is cited by
-
Association between serum S100A11 levels and glucose metabolism in diabetic process
Diabetology & Metabolic Syndrome (2023)
-
Young-onset colorectal cancer
Nature Reviews Disease Primers (2023)
-
Haemoglobin A1c and serum glucose levels and risk of gastric cancer: a systematic review and meta-analysis
British Journal of Cancer (2022)
-
Prognostic Significance of VEGF and HIF-1 α in Hepatocellular Carcinoma Patients Receiving Sorafenib Versus Metformin Sorafenib Combination
Journal of Gastrointestinal Cancer (2021)
-
High glucose: an emerging association between diabetes mellitus and cancer progression
Journal of Molecular Medicine (2021)
