Article Text

Abstract
Objective: To determine in a prospective population-based cohort study relationships between different measures of body mass and the incidence of severe knee and hip osteoarthritis defined as arthroplasty of knee or hip due to osteoarthritis.
Materials and methods: Body mass index (BMI), waist circumference, waist–hip ratio (WHR), weight and percentage of body fat (BF%) were measured at baseline in 11 026 men and 16 934 women from the general population. The incidence of osteoarthritis over 11 years was monitored by linkage with the Swedish hospital discharge register.
Results: 471 individuals had knee osteoarthritis and 551 had hip osteoarthritis. After adjustment for age, sex, smoking and physical activity, the relative risks (RR) of knee osteoarthritis (fourth vs first quartile) were 8.1 (95% CI 5.3 to 12.4) for BMI, 6.7 (4.5 to 9.9) for waist circumference, 6.5 (4.6 to 9.43) for weight, 3.6 (2.6 to 5.0) for BF% and 2.2 (1.7 to 3.0) for WHR. Corresponding RR for hip osteoarthritis were 2.6 (2.0 to 3.4) for BMI, 3.0 (2.3 to 4.0) for weight, 2.5 (1.9 to 3.3) for waist, 1.3 (0.99 to 1.6) for WHR and 1.5 (1.2 to 2.0) for BF%.
Conclusion: All measures of overweight were associated with the incidence of knee osteoarthritis, with the strongest relative risk gradient observed for BMI. The incidence of hip osteoarthritis showed smaller but significant differences between normal weight and obesity. Our results support a major link between overweight and biomechanics in increasing the risk of knee and hip osteoarthritis in men and women.
Statistics from Altmetric.com
The relationship between overweight and obesity and an increased risk of knee and hip osteoarthritis has been documented in several previous studies, in particular for the knee.1–9 For the hip, the evidence is inconsistent, some studies finding an association, others not, with the association appearing stronger for case definitions based on symptoms than on radiological findings.6 8–23
The increased risk of osteoarthritis associated with overweight and obesity is suggested to have a significant biomechanical component, but an additional role for metabolic factors associated with adipose tissue was suggested.24 There are several different measures of overweight and obesity, eg, body mass index (BMI), waist circumference, waist–hip ratio (WHR) and percentage of body fat (BF%). Even though these measures are positively related to each other, the correlations are sometimes quite low and the measures reflect different aspects of body mass and adipose tissue distribution and type. The latter aspect is of interest in light of the suggested connection between osteoarthritis and metabolically active adipose tissue.24 Few studies have explored whether the different measures of overweight differ in their relationships with knee or hip osteoarthritis, and they have generally used osteoarthritis as defined on plain radiographs for case identification,3 5 11 or assessed cartilage volume by magnetic resonance imaging.25 The relevance of radiographically defined osteoarthritis in terms of symptomatic disease burden or health economics is uncertain. None of these studies have included both knee and hip osteoarthritis.
The purpose of this large population-based, prospective cohort study was to compare the relationships between different measures of body mass and the incidence of arthroplasty due to knee or hip osteoarthritis in men and women, a measure of significant symptomatic and economic osteoarthritis disease burden.
METHODS
Study population
All men and women living in the city of Malmö in Sweden, who were born between 1923 and 1945 (men) or between 1923 and 1950 (women), were invited to participate in the Malmö Diet and Cancer (MDC) study. The subjects were invited by letters and advertisements in newspapers. Between March 1991 and September 1996, the respondents participated in a baseline examination with different clinical examinations at the screening centre and filled in a self-administered questionnaire. The cohort consisted of 28 449 subjects (11 246 men and 17 203 women) from the eligible population of approximately 74 000 individuals. The characteristics of all participants and non-participants have been reported.26 It was shown that the cohort was representative of the eligible population with respect to the prevalence of overweight, smoking, educational level, type of employment and marital status.26 However, the mortality rate was higher in non-participants. On 1 January 1991, the age of the participants was 54.9 years (SD 7.6) and the age of non-participants was 54.3 years (SD 7.8); 39.4% of participants and 43.6% of non-participants were men. Of the 28 449 participants, 185 were excluded from the present study due to incomplete anthropometric or body fat data. Another 304 subjects who had been surgically treated due to knee or hip osteoarthritis before the baseline examination were excluded. The research ethical committee at Lund University approved the MDC study (LU 51–90). Each participant signed a written informed consent.
Baseline examinations
Body weight, height, waist and hip circumferences were measured at the screening centre. The examinations were performed by two trained nurses. Standing height was measured with a fixed stadiometer calibrated in centimetres. Weight was measured to the nearest 0.1 kg using a balance beam scale with subjects wearing light clothing and no shoes. BMI was calculated as weight in kilograms divided by height squared in metres. Waist was measured as the circumference (in centimetres) between the lowest rib margin and the iliac crest and hip circumference (in centimetres) as the largest circumference between the waist and thighs. WHR was defined as the ratio of the circumference of waist to hip. Weight at 20 years of age was assessed in the questionnaire. A total of 24 166 subjects (86%) filled in this question. A bioelectrical impedance method was used to measure body composition. The BF% was calculated using an algorithm according to procedures provided by the manufacturer (BIA 103, single-frequency analyser; RJL Systems, Detroit, USA).27
A self-administered questionnaire was used to assess medical history and lifestyle factors. Subjects were categorised into current smokers (ie, those who smoked regularly or occasionally) or non-smokers (ie, former smokers and never smokers). Information on physical activities in leisure time was explored through 18 questions covering a range of activities in the four seasons.28 29 The scores were divided into quartiles of physical activity when used in the analysis.29 Information about smoking or physical activity was missing for 505 (1.8%) of the subjects.
The subjects reported whether they had been treated for different medical problems, eg, myocardial infarction, stroke, cancer, peripheral arterial disease, hypertension, diabetes, goiter, gastric ulcer, asthma or chronic obstructive pulmonary disease, inflammatory bowel disease and renal stones. Subjects with history of any of these diseases were excluded in a separate analysis to examine the influence on the risk of arthroplasty.
Definition of knee and hip osteoarthritis
The follow-up times were calculated separately for knee and hip. All participants were followed until the first osteoarthritis surgery, emigration from Sweden, death or 31 December 2005, whichever came first. Information on knee and hip arthroplasty for osteoarthritis and mortality were based on record linkage with the national Swedish hospital discharge register and the Swedish causes of death register. Subjects who moved out of Sweden were censored at the day of emigration.
Knee osteoarthritis was defined as a first knee arthroplasty or high tibial osteotomy (procedures coded 8424, 8423, 8428, 8010, 8199 or NGB09, NGB19, NGB29, NGB39, NGB49, NGB99 and NGK59) in combination with a contemporaneous diagnosis of osteoarthritis (715 or M17 according to the International Classification of Disease (ICD) 9 and ICD-10, respectively). Only the first event was counted for patients with more than one knee arthroplasty.
Hip osteoarthritis was defined as a first hip arthroplasty (procedures coded 8414, 8010, NFB09, NFB19, NFB29, NFB39, NFB49 and NFB99) in combination with a contemporaneous diagnosis of hip osteoarthritis (715 or M16 according to ICD-9 and ICD-10, respectively). Patients with more than one hip arthroplasty were only counted once. Cases coded with a diagnosis of primary unilateral osteoarthritis constituted 93% and 96% of all knees and hips included, respectively.
Statistics
Pearson’s correlations were used to assess the covariation between the anthropometric measures. Kaplan–Meier curves were created to illustrate the crude incidence rates of knee and hip osteoarthritis over time. Cox’s proportional hazards model was used to assess the incidence of surgery as a result of knee or hip osteoarthritis, in relation to measures of body mass, with adjustments for confounding factors. Potential confounding factors were selected from those available based on a priori assumptions of risk factors for osteoarthritis.1 7 17 The fit of the proportional hazards model was confirmed by plotting the incidence of osteoarthritis over time for the different categories of risk factors. The anthropometric measures were divided into sex-specific quartiles before analysis. Age was entered as a continuous variable. Smoking was used as a dichotomous variable. Physical activity was categorised into quartiles in the regression analysis. All comparisons were two-sided and a 5% level of significance was used.
RESULTS
Study cohort
The study population characteristics are presented in table 1.
Weight and BMI were highly correlated in both men and women. WHR showed moderate or low correlations with BMI, weight and BF% (table 2).
Incidence of knee osteoarthritis arthroplasty
A total of 27 960 subjects was available for the analysis of the incidence of osteoarthritis. Of them, 421 were treated with knee arthroplasty or high tibial osteotomy (n = 50) as a result of osteoarthritis during the follow-up of 11.2 years (0–14.8) (median 11.3, interquartile range 10.2–12.8). BMI, weight, waist, WHR and BF% were significantly related to knee osteoarthritis in both sexes, with the strongest association between BMI and arthroplasty/osteotomy (table 3). For example, the adjusted RR for men with BMI in the fourth quartile was 7.0 (3.3 to 14.8) and for women 8.7 (5.2 to 14.6).
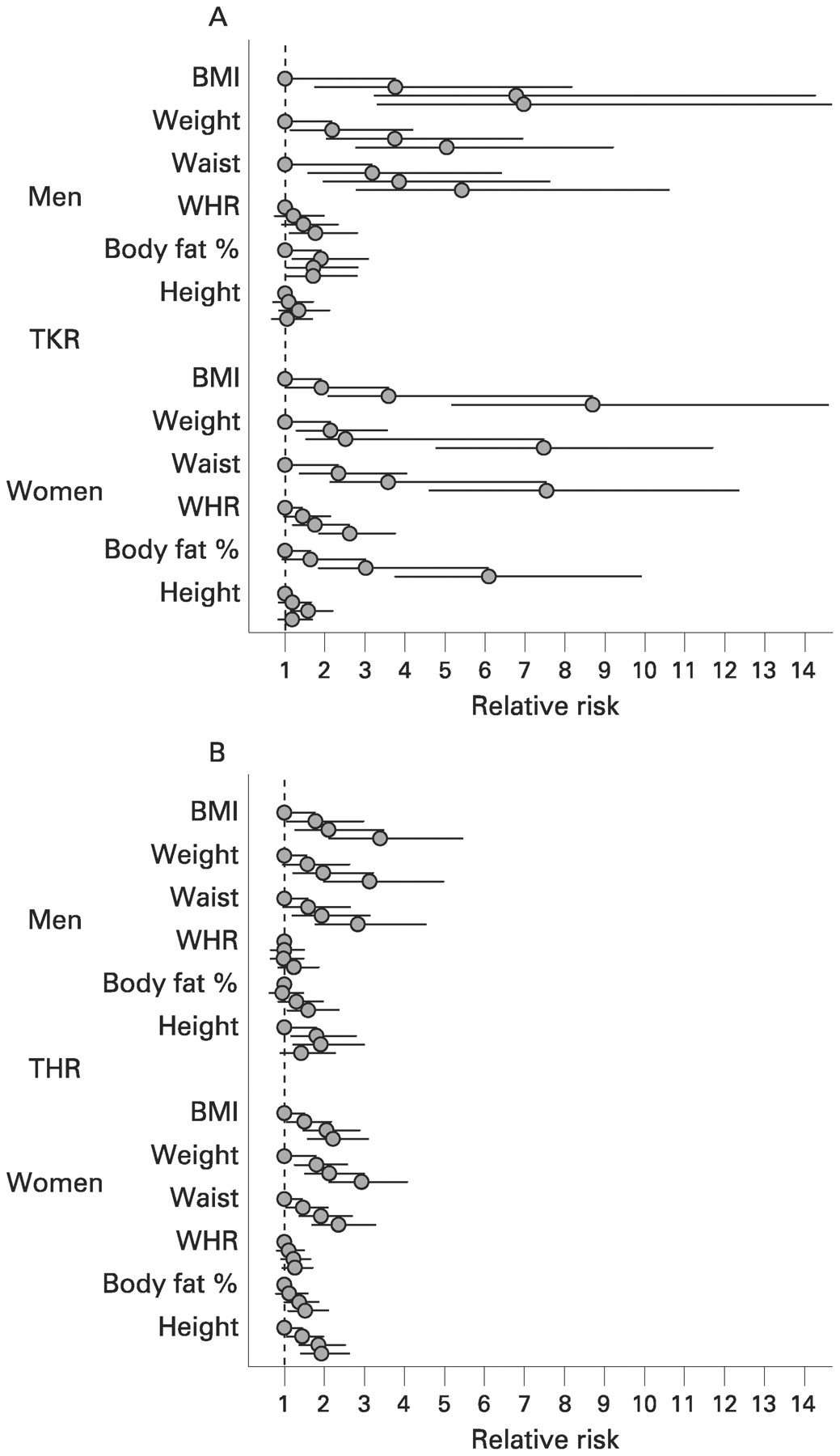
When compared with subjects with BMI less than 25 kg/m2, the RR for men with BMI 25–30 kg/m2 and BMI greater than 30 kg/m2 were 3.1 (2.0 to 4.9) and 4.4 (2.6 to 7.5), respectively, and for women 2.8 (2.0 to 3.9) and 6.9 (5.0 to 9.6), respectively (fig 1). In women, a dose–response gradient between BF% and RR for total knee replacement was apparent, but less so for men (fig 1).

Adjusted relative risks (RR) for men and women for total knee replacement (TKR) or osteotomy for severe knee osteoarthritis (top), or total hip replacement (THR) for severe hip osteoarthritis (bottom). Error bars show 95% CI for RR estimates; each group of four symbols represent quartiles 1 to 4. The dotted line corresponds to RR 1. BMI, body mass index; WHR, waist–hip ratio.
In men, there was no significant relationship between height and knee osteoarthritis. In women, a non-linear relationship between height and knee osteoarthritis was observed, with an increased incidence in the third quartile, whereas for men there was no such relationship (fig 1).
Incidence of hip osteoarthritis arthroplasty
A total of 551 was treated with hip arthroplasty as a result of osteoarthritis during the follow-up. BMI, weight and waist were significantly associated with hip osteoarthritis (table 4). These relationships were similar in men and women (fig 1). The gradient over the quartiles of BF% was weaker, but statistically significant. For WHR, the relationship with hip osteoarthritis was non-significant both in men and women (fig 1).
When compared with subjects with BMI less than 25 kg/m2, the RR for men with BMI 25–30 kg/m2 and BMI greater than 30 kg/m2 were 1.6 (1.1 to 2.3) and 3.3 (2.2 to 5.0), respectively, and for women 1.4 (1.1 to 1.8) and 2.1 (1.6 to 2.7), respectively.
In men, there was a non-linear relationship between height and hip osteoarthritis (fig 1). In women, the RR of hip osteoarthritis increased gradually over the quartiles of height.
Incidence of severe osteoarthritis in relation to weight at age 20 years
Information about self-reported weight at the age of 20 years was available for 24 008 subjects, 9341 men and 14 667 women (table 4). Weight at 20 years was significantly associated with knee osteoarthritis after adjustments for age, sex, smoking and physical activity. However, this relationship was attenuated and non-significant after adjustment for BMI measured at the baseline examination at the median age of approximately 60 years. In contrast, both weight at 20 years and BMI at the examination were significant risk factors for hip osteoarthritis, after mutual adjustments in the multivariate regression (table 5).
Influence of co-morbidities on relationships between body mass and osteoarthritis
To explore whether a healthy patient selection effect on the arthroplasty or osteotomy decision could influence the relationships between body mass and osteoarthritis, individuals with a self-reported history of myocardial infarction, stroke, cancer, peripheral arterial disease, hypertension, diabetes, goiter, gastric ulcer, asthma or chronic obstructive pulmonary disease, inflammatory bowel disease and renal stones were excluded from the analyses. A total of 15 287 subjects remained, 209 of them had arthroplasty or osteotomy for knee osteoarthritis and 272 had arthroplasty for hip osteoarthritis during the follow-up. In this group, the adjusted RR of knee osteoarthritis for those with BMI in the top quartile was 14.9 (6.8 to 32.4). The adjusted RR for hip osteoarthritis was 2.4 (1.6 to 3.5) for those with BMI in the top quartile.
DISCUSSION
Previous studies have reported on the risk of knee or hip osteoarthritis in subjects with overweight or obesity. Whereas the reported relationship between overweight measures and knee osteoarthritis has been consistent, it has been inconsistent for the hip. To our knowledge no report has in the same population compared the incidence of severe knee and hip osteoarthritis in men and women in relation to different measures of overweight and used an outcome tightly linked to the disease burden of severe osteoarthritis. The results from this large, prospective population-based cohort study show that BMI, weight and waist circumference were major risk factors for knee arthroplasty or osteotomy as a result of osteoarthritis, with the highest RR for subjects with BMI in the top quartile (fig 1 and fig 2). BF% was associated with knee osteoarthritis mainly in women and WHR showed substantially weaker associations with the incidence of knee osteoarthritis. All measures related to overweight showed weaker associations with the incidence of severe hip osteoarthritis than with severe knee osteoarthritis. However, BMI, weight and waist were also important risk factors for osteoarthritis of the hip leading to arthroplasty. These relationships held true for both men and women.

{kind=link}
{kind=link}
Kaplan–Meier survival analysis of knee and hip. Graphs show study population fractions without total knee replacement (TKR) or osteotomy for osteoarthritis (A, top), and study population fraction without total hip replacement (THR) for osteoarthritis (B, bottom). For each panel, the four plots represent from top to bottom body mass index (BMI) quartiles 1 to 4, with a significant difference between each of the four curves in the upper and lower panels. The adjusted relative risks are given in table 3 and table 4. Median BMI values for the quartiles are given in table 3.
It was suggested that metabolic or inflammatory factors contribute to the relationships between obesity and knee osteoarthritis.24 Many studies have reported that, for example, BF% or WHR are more closely linked to inflammation and metabolic factors than BMI, particularly in women.30 The fact that BMI was associated with much higher point estimates than were WHR or BF% suggests that mechanical factors associated with overweight are more strongly related to knee and hip osteoarthritis than metabolic or inflammatory factors. However, all measures of overweight are very unspecific surrogate measures of inflammation, and the present results do not exclude a role of systemic or local inflammatory and metabolic factors associated with adipose tissue as contributors to the risk of knee or hip osteoarthritis. It is of interest here to note the stronger relationship between BF% and severe knee and hip osteoarthritis for women than for men (fig 1). The effect of BMI may be modified by other risk factors, such as sex, joint malalignment and joint injury.22 23 31–34 Whether the influence of weight varies with other predisposing factors remains to be determined.
In the present study, we used a case definition of total arthroplasty or high tibial osteotomy of the knee or arthroplasty of the hip due to osteoarthritis. Other studies that have explored the relationship between obesity and osteoarthritis have used as case definitions these same criteria, or knee or hip arthroplasty without a confirmed diagnosis, osteoarthritis diagnosed by variable radiographic criteria, osteoarthritis defined by symptom criteria, or by self-reported diagnosis. The relationship between these different osteoarthritis definitions is uncertain, and their relationship with obesity may not be the same, explaining some of the variability in the published results.35 Although the definition of arthroplasty or osteotomy due to osteoarthritis will only identify the tip of the iceberg of the very large osteoarthritis population, it has the advantage of an unambiguous connection with the disease burden of osteoarthritis and being available in reliable national registries. Additional reasons for the variable results of previous studies include variations in study design, focus on different population subsets such as men or women, or occupation and duration of follow-up. Our finding that in the same population the association between BMI and severe hip osteoarthritis was weaker than that between BMI and severe knee osteoarthritis suggests that some previous studies failing to show the association with hip osteoarthritis may have been underpowered.
The national Swedish hospital discharge register was used for case retrieval. This register has been active during the entire follow-up period, it covers all Swedish hospitals, has been validated against the national Swedish arthroplasty registers and was estimated to include at least 95% of primary knee and hip arthroplasties.36 Misclassification of diagnosis may represent a source of bias. Primary osteoarthritis was the diagnosis for more than 85% of all primary knee arthroplasties and more than 75% of all primary hip arthroplasties in Sweden during the follow-up period. The proportion of diagnostic misclassification was estimated at approximately 5% for hip replacements.36 We therefore suggest that the bias in the present study due to the misclassification of contemporaneous osteoarthritis is small and probably non-differential.
The decision to treat a patient with osteoarthritis surgically is influenced by a number of factors in addition to those related to the severity of symptoms and radiographic signs.37 Of particular relevance to this and other studies using arthroplasty is the possibility of a healthy patient selection bias in the decision to perform an arthroplasty. In our analyses we found that the strong relationships between overweight measures and arthroplasty for osteoarthritis remained following the exclusion of participants with self-reported significant co-morbidities at the baseline examination. This would argue against a healthy patient selection bias influencing our results.
The participant rate in MDC was approximately 41%, and it may be questioned whether the study cohort is representative of the source population. It was shown that BMI, the prevalence of smoking and sociodemographic status in the study cohort was similar to that of the source population, based on a mailed questionnaire to the source population in which the response rate was approximately 75%.26 Similar to most cohort studies, the mortality rates were higher in non-participants than in participants.
The large size of the cohort and the prospective design are major strengths of the study. Subjects with knee or hip surgery for osteoarthritis before the baseline examination were not included, excluding a major proportion of individuals with severe knee or hip osteoarthritis already at baseline. A limitation is that we could not exclude all subjects with any baseline knee or hip pain for lack of complete baseline data on these symptoms. Therefore, the cases reported here may include some who already had osteoarthritis at baseline. However, we monitored a proxy for severe symptomatic osteoarthritis: the incidence of knee or hip arthroplasty as a result of osteoarthritis. Even though the prospective design minimised the risk of reverse causality, it is possible that pain in the knee or hip in some cases may already have influenced health behaviour at the baseline examination.
Our results extend those of previous reports by comparing within the same large population-based study risks for severe knee and hip osteoarthritis in both men and women, using several different measures of overweight. We conclude that all measures of overweight were significantly associated with the incidence of severe knee osteoarthritis in men and women, and the strongest relative risk gradient was observed for BMI. Even though the incidence of severe hip osteoarthritis showed smaller differences between normal weight and obesity than for the knee, body mass was also an important risk factor for severe hip osteoarthritis in men and women, consistent with some recent reports.17 20 There appeared to be a continuous dose–response relationship between BMI and the risk of arthroplasty for osteoarthritis. A significant risk increase for both knee and hip osteoarthritis, after adjustment for age, sex, smoking and physical activity, was already apparent for the second BMI quartile, corresponding to a median BMI of 25 for men and 23.6 for women.
REFERENCES
Footnotes
Competing interests: Declared. MG, JR and GE are employees of AstraZeneca. LSL and PMN have no conflicts of interest to report.
Funding: This study was supported by AstraZeneca R&D, the Swedish Research Council, the Medical Faculty of Lund University, Region Skåne, the Swedish Rheumatism Association and the King Gustaf V 80th Birthday Fund.
Ethics approval: The research ethical committee at Lund University approved the MDC study (LU 51–90).
Patient consent: Obtained.