Article Text

Abstract
AIM To establish the prevalence, severity, and risk factors for diabetic retinopathy in a representative sample of Victorian residents aged 40 years and older.
METHODS A population based, cluster sampling method was used to recruit 4744 participants (86% participation rate). Nine randomly selected, suburban Melbourne clusters and four randomly selected, rural Victorian clusters were used. Participants provided a detailed medical and personal history and underwent an ocular examination including funduscopy and fundus photography. Rural participants provided a blood sample, from which the glycosylated haemoglobin percentage was measured. The diagnosis of diabetic retinopathy was based on fundus photographs from participants with self reported diabetes.
RESULTS The prevalence of diabetic retinopathy among people with self reported diabetes was 29.1%. The prevalence of untreated, vision threatening retinopathy was 2.8%. Retinopathy was positively associated with a longer reported duration of diabetes diagnosis (p<0.01) and with higher fractions of glycosylated haemoglobin (p<0.01). Retinopathy was not significantly associated with age, ethnicity, body mass index, glaucoma, myopia or intake of alcohol, tobacco, or aspirin (all p > 0.05).
CONCLUSIONS Most people in Victoria with proliferative diabetic retinopathy or clinically significant macular oedema have received laser treatment. There remains however, a small but important group who have not received treatment and whose vision is threatened. People with diabetes should be encouraged to maintain strict glycaemic control and to undergo regular screening to delay or prevent the development of retinopathy.
- diabetic retinopathy
- prevalence
- risk factors
Statistics from Altmetric.com
Diabetic retinopathy is the most common chronic complication of diabetes1 and one of the most devastating. In the USA it has been estimated that diabetic retinopathy (DR) is the most common cause of new cases of blindness in people aged 25–74 years.1
The Visual Impairment Project (VIP)2 is a large, population based epidemiological study which is ongoing in the state of Victoria, Australia. It has been designed to investigate the distribution and determinants of eye disease, the impact of blindness and visual impairment on individuals, and the use of and barriers to eye healthcare services. This report analyses the epidemiology of DR using cross sectional data collected during the baseline phase of the project between 1992 and 1996.
We report the prevalence of DR, based on fundus photographs from participants with self reported diabetes. This includes an evaluation of the prevalence of vision threatening DR as well as previous laser treatment for DR. We also demonstrate in our cohort, the well established3 association between both duration and control of diabetes and the prevalence of retinopathy.
Methods
A stratified cluster sampling method was used to select participants. Each cluster consisted of two adjacent census collector districts. The urban component of the project contained nine randomly selected Melbourne suburban clusters. The rural component contained four randomly selected clusters from throughout the rest of the state.
A private household census was conducted to identify permanent household members aged 40 years or older who were classified as eligible residents. A screening questionnaire was then administered in the home to establish contact with eligible residents and to determine basic demographics. When respondents were not available, repeated visits were made to the home. Eligible residents were then invited to attend a local temporary test site for a more comprehensive interview and an ophthalmic examination. Those who were unable to attend the test site were offered a modified home visit so that as much information as possible could be obtained.
At the test site, another interview was conducted by trained interviewers. It elicited further demographic details, a history of medical and ocular health, a history of smoking and alcohol intake, and a history of medication use. Participants were classified into various ethnic groups on the basis of their report of their parents' country of birth. Body weight and height were questioned and body mass index (BMI) was calculated as weight (kg)/(height (m)2).
The interview included specific questioning about whether participants had ever been diagnosed with diabetes mellitus and the year in which such a diagnosis was made. Participants with previously diagnosed diabetes were also asked if and when their last dilated fundus examination had been conducted and who performed the examination. The questions relating to diabetes have been previously employed and validated by Welborn et al.4
Participants underwent a detailed examination of each eye. Pupils were dilated with one drop of tropicamide (0.5%) and one drop of phenylephrine hydrochloride (10%). Stereoscopic fundus photographs were then taken with a Topcon TRC fundus camera (Topcon, Paramus, NJ, USA). Two 30 degree fields of the fundus were photographed in each eye; one centred on the optic disc and the other centred on the fovea. Photographs from participants who reported having diabetes were evaluated by an ophthalmologist with medical retina subspecialist qualifications. This evaluation was used to establish the presence or absence of any diabetic retinopathy (DR), proliferative retinopathy, clinically significant macular oedema (as defined by the Early Treatment Diabetic Retinopathy Study (ETDRS)5), and previous retinal laser treatment. Levels of diabetic retinopathy were defined, according to the Academy of Ophthalmology in the United States, as mild non-proliferative, moderate non-proliferative, severe non-proliferative, and proliferative DR.6
Dilated funduscopy was performed by an ophthalmologist with a 90 dioptre hand held fundus viewing lens used at a Topcon SL slit lamp (Topcon). This was supplemented by indirect ophthalmoscopy if peripheral abnormalities were revealed or suspected. The presence or absence of any DR, proliferative retinopathy, clinically significant macular oedema, or previous retinal laser treatment was recorded.
In this report, DR status is assessed only in participants with self reported diabetes. Assignment of DR status is based on fundus photographs where they are available. In 14 participants for whom fundus photographs were not available, the findings from dilated funduscopy have been used to determine DR status. Two participants who reported having diabetes refused fundus photography and fundus examination but allowed us to obtain information about DR status from their ophthalmologist.
All participants at rural test sites were asked to provide a fingerprick blood sample. This was used to measure glycosylated haemoglobin percentages (HbA1c), via a Bayer DCA2000 HbA1c analyser (Bayer Co, Elkhart, IN, USA). This device has a measurable range of HbA1c from 3.9% to 14.0%. A reading of 14.0% was found in three participants who all reported a diagnosis of diabetes and was entered as the actual level. A reading of 3.9% was found in one participant who reported no diagnosis of diabetes and was entered as the actual level.
Glaucoma status was determined by the following method. Intraocular pressure was measured with a hand held applanation tonometer (Oculab Tonopen, Oculab, La Jolla, CA, USA). In participants with Tonopen readings ⩾ 22 mm Hg in either eye, pressure was checked with Goldmann applanation tonometry. A Humphrey computerised visual field analyser (Humphrey Instruments, Dublin, CA, USA) was used to record 24-2fastpac visual fields in all participants. Participants who were unable reliably to complete computerised visual field assessments underwent Bjerrum visual field testing. Glaucoma status was evaluated by a consensus panel comprising six ophthalmologists, including two glaucoma specialists. This panel determined glaucoma status on the basis of Humphrey visual fields and photographs of the optic disc. All participants with a cup/disc ratio that was enlarged (⩾0.7) or asymmetrical (⩾0.3 interocular difference), a glaucomatous visual field defect, or an intraocular pressure of greater than 21 mm Hg in either eye were presented to the panel.7
The presence of myopia was determined as follows. Presenting visual acuity was determined with an ETDRS 4 metre chart. Any spectacle correction worn was measured with a Humphrey automatic lens analyser (model 330, Humphrey Instruments, Dublin, CA, USA). A Humphrey automatic refractor (Humphrey Instruments) was used to measure the objective refraction in all participants who read fewer than 53 letters (6/7.5 or 20/25) in either eye. This was then refined by participative refraction. Myopia was defined as a best corrected minus spherical equivalent of more than −0.5 dioptres in either eye.
Double entry of data with comparison was used to minimise errors in the data set. Statistical analyses were performed using sasversion 6.09 (SAS Institute Inc, Cary, NC, USA). The statistical procedures used in this research include summary statistics,t tests, χ2 analyses, and multiple logistic regression. These procedures are documented in theSAS/STAT Users' Guide.8 A p value of <0.05 was considered to be statistically significant.
The Royal Victorian Eye and Ear Hospital human research and ethics committee approved the project. Informed consent was obtained from all participants.
Further details about the methodology of the urban component of the VIP are published elsewhere.2 For the purposes of this report, the sampling and study methods used in the rural component of the VIP were the same except that glycosylated haemoglobin measurements were added. A comparison of participants with non-participants from the urban component of the VIP has also been published.9
Results
In total, 5520 participants were identified as being eligible to participate in the rural and urban components of the VIP. Of these, 776 did not participate, giving a response rate of 86%. In the urban clusters, the overall response rate was 84% (3271/3912). In the rural clusters, the overall response rate was 92% (1473/1608).
The prevalence of self reported diabetes was 5.1% (239/4478). This did not differ significantly between the urban and the rural samples (5.2% and 4.9% respectively, p=0.69). The number of participants who reported using medications to control their diabetes was 172 (72%). There were 39 participants who used insulin (16.6%) and 133 participants who used oral hypoglycaemic agents (56.6%). This includes four participants who reported using both insulin and oral hypoglycaemics. A further four participants reported using medications for diabetes control but did not report what these medications were.
We have analysed the fundus photographs from both eyes of 215 of the 239 people in our cohort who reported a diagnosis of diabetes. In three participants there was a photograph of one eye only, which showed evidence of DR. In 14 of the remaining participants without photographs, information was available from indirect ophthalmoscopy. For two participants there were no photographs or funduscopy but information was available from a treating ophthalmologist that DR was present in at least one eye. Thus, we have reliable information about the presence or absence of DR in either eye from 234 of the 239 people with self reported diabetes.
The prevalence of DR among people with self reported diabetes was 32.3% (53/164) in the urban sample and 21.4% (15/70) in the rural sample. As this difference was not statistically significant (p = 0.10), we have combined information from the two samples. This gives an overall prevalence of DR among people with self reported diabetes of 29.1% (68/234).
The prevalence of DR in men was 29.5% (35/135), which was not significantly different from the prevalence in women of 33.3% (33/99) (p=0.22). The mean age of participants with DR was 64.2 years (median 63.5, range 45–91). The mean age of participants with self reported diabetes but without DR was 64.6 years (median 65.0, range 42–84). The prevalence of DR did not vary significantly with age (p= 0.22).
The prevalence of DR in participants who reported a diabetes diagnosis before the age of 30 was 50.0% (4/8). The prevalence of DR in participants who reported a diabetes diagnosis at the age of 30 or older was 28.3% (64/226). This difference was not statistically significant (p=0.18).
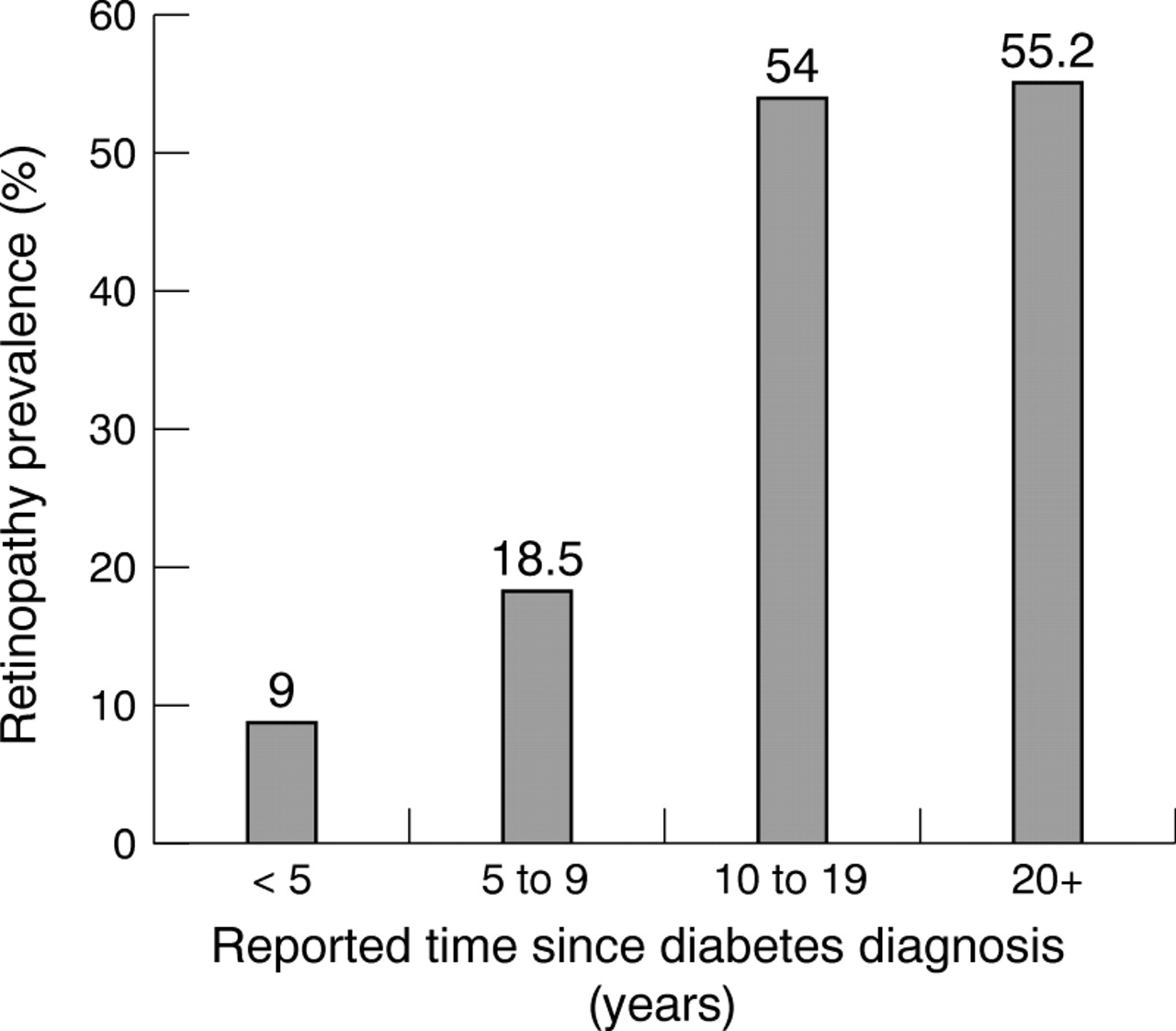
The mean reported duration of diabetes diagnosis in participants with DR was 14.6 years (median 14.0, range 0–44). The mean reported duration of diabetes diagnosis in participants without DR was 6.8 years (median 5.0, range 0–57). This difference was statistically significant (p < 0.01). Figure 1 summarises DR prevalence in different categories of reported diabetes duration.

Prevalence of retinopathy by reported duration of diabetes diagnosis.
We have glycosylated haemoglobin measurements for 70 participants with self reported diabetes, 15 of whom had diabetic retinopathy. The mean HbA1c in participants with DR was 9.3% (median 9.1, range 7.0–14.0). The mean HbA1c in participants without DR was 7.2% (median 6.9, range 4.7–14.0). This difference was statistically significant (p<0.01). Figure 2 summarises DR prevalence in different categories of HbA1c measurement.

{kind=link}
{kind=link}
Prevalence of retinopathy by glycosylated haemoglobin level.
The prevalence of DR in participants who reported using insulin was 67.6% (25/37). The prevalence of DR in those who reported using oral hypoglycaemic agents without insulin to control their diabetes was 29.9% (38/127). The prevalence of DR in participants who reported using no diabetes medications was 7.5% (5/67).
Among people with self reported diabetes, no statistically significant difference could be found between participants with DR and those without DR in terms of ethnicity, body mass index, glaucoma, myopia, alcohol intake, tobacco intake, aspirin use (current), or antihypertensive use (current or ever) (data not presented).
To examine the treatment and severity of DR, we only included the 215 participants with self reported diabetes for whom we had graded fundus photographs from both eyes. There were 14 participants with evidence of laser treatment (6.5%) and this was bilateral in nine of these (4.2%). There were 12 people who had clinically significant macular oedema (5.6%) and this was bilateral in five of these (2.3%). Untreated clinically significant macular oedema was found in five participants, including one person with bilateral untreated clinically significant macular oedema and one person with treated macular oedema in the fellow eye. There were nine people with proliferative DR (4.2%) and this was bilateral in five of these (2.3%). Only one participant had untreated proliferative DR. This participant had treated proliferative DR in the other eye and did not have macular oedema. Combining this information gives six people (2.8%) with untreated, vision threatening DR including one person with bilateral, untreated, vision threatening DR (0.47%). The prevalence of mild, moderate, and severe non-proliferative DR was 16.7% (n=37), 6.8% (n=15), and 0.5% (n=1), respectively.
The duration of diabetes diagnosis in the 12 participants with clinically significant macular oedema ranged from 4 years to 30 years with a median of 17.5 years and a mean of 17.7 years. The duration of diabetes diagnosis in the nine participants with proliferative DR ranged from 10 years to 38 years with a median of 18 years and a mean of 20.1 years.
One hundred and thirty one participants (64%) reported having had a dilated fundus examination at least once. Participants taking insulin were far more likely to have ever had a retinal examination (91% versus 59%, χ2 =12.4, p=0.001). In a multivariate logistic regression model with backwards selection that included age, sex, years since diabetes diagnosis, insulin treatment, born outside Australia, and English spoken at home, the following variables were found to be significantly associated with never having had a retinal examination: born outside Australia (OR=2.24, 95%CL=1.23, 4.08) and not treated with insulin (OR=6.67, 95%CL=1.93, 22.7).
One hundred and ninety five participants could recall the year of their last retinal examination. Of them, the percentage who had a retinal examination within the past 2 years by level of DR was: none, 49.3%; mild non-proliferative retinopathy, 41.4%; moderate non-proliferative retinopathy, 83.3%; severe non-proliferative retinopathy, 0%; proliferative retinopathy, 55.6%. Participants who had any DR were not more likely to have had a retinal examination in the previous 2 years than participants without DR (52.9% versus 49.3%, χ2=0.20, p=0.66). People treated with insulin were significantly more likely to have had a dilated fundus examination in the previous 2 years than people treated with diet and/or tablets (69.7% versus 48.0%, χ2 =5.24, p=0.02).
Among participants who reported no previous diagnosis of diabetes, there were no signs of DR found in any individual at the clinical eye examination.
Discussion
Our estimate of the prevalence of DR in people with self reported diabetes is 29%. This is similar to the prevalence found in other population based studies. The Blue Mountain Eye Study (BMES)10 found a DR prevalence of 32% among 253 people with diabetes aged 49 or older in western Sydney. This estimate included 38 people who were newly diagnosed with diabetes by the study group (fasting blood glucose ⩾7.8). The largest Australian study of DR to date is the Newcastle Diabetic Retinopathy Study.11This was a longitudinal, clinic based study of people with diabetes of all ages, which was conducted over an 11 year period. An overall 35% prevalence of any signs of DR was reported at the conclusion of the study. The Beaver Dam Eye Study (BDES),12 from Wisconsin, USA, examined a population aged from 43 to 84 years. Their estimate for DR prevalence in 435 people with diabetes was 37%. This included 49 people who were newly diagnosed with diabetes by the study group (using HbA1c levels). The Rotterdam study13 was a population based investigation of people aged 55 years or older in Holland which included a glucose challenge test for participants who were not taking antidiabetes medications. Their estimate of the prevalence of DR among people with diabetes was 26%. The Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR)1investigated people with diabetes of all ages who were identified by primary care physicians. They found DR prevalence rates of 71% (type 1 diabetes) and 39% (type 2 diabetes). This group has also published a summary of DR prevalence and incidence data from other population based studies conducted before 1989.1
Variation in the photographic methods used to identify DR may at least partially explain the variation in prevalence between these studies. The WESDR1 and Newcastle11 studies used all seven of the standard 30 degree fields originally described in the Diabetic Retinopathy Study (DRS).14 The BMES10 used fields 1 to 5 (inclusive) and the BDES12 used fields 1, 2, and 3. These studies all found slightly higher prevalence rates than ours, which were based on only two 30 degree fields. (Our fields were centred on the disc and on the macula and thus are equivalent to DRS standard fields 1 and 2 respectively). In contrast, the Rotterdam study,13 which found lower prevalence rates than ours, used only one 35 degree field, centred on the macula. Moss et alinvestigated the effect on sensitivity of DR detection when a smaller area of the retina is examined.15 Using all 7 DRS standard fields as their gold standard, they found 87% sensitivity for detecting any retinopathy when only fields 1 and 2 are used as in our study and 95% sensitivity when only fields 1–4 are used.
Our data indicate an association between longer duration of diabetes and increased prevalence of retinopathy. The WESDR has shown that non-proliferative retinal lesions, macular oedema, and proliferative DR each have a prevalence that is strongly associated with the duration of diabetes diagnosis.3 16 17 Other large epidemiological studies have also supported such associations.10 12 18 19 The Newcastle Diabetic Retinopathy Study reported that among participants with diabetes but without retinopathy, 8% developed retinopathy each year.11
Our findings also demonstrate a correlation of lower HbA1clevels with a lower prevalence of DR. An association between tighter diabetes control and lower DR prevalence has been consistently found in other large epidemiological studies.13 18 20 21 The WESDR found that higher HbA1c levels were positively associated with prevalence rates for non-proliferative lesions, proliferative DR, and macular oedema and that HbA1cpredicts both the incidence and progression of retinopathy.3 16 17 22 The strongest available evidence comes from the Diabetes Control and Complications Trial (DCCT).23 This was a large, randomised clinical trial of participants with young onset insulin dependent diabetes mellitus (IDDM). It showed that the risk and progression of retinopathy can be reduced by intensive diabetic therapy, aiming to maintain near normal serum glucose levels. A 10% lower HbA1c (for example, 8% versus 7.2%) was associated with a 43% to 45% lower risk of progression of retinopathy. The study concluded that there was no level of HbA1c below which the risk of DR was completely eliminated. However, Warram et al used DCCT and WESDR data to suggest that in patients with IDDM, there may be a threshold value of HbA1c of around 8.5%, above which the risk of DR progression increases rapidly.24
There was a dramatic variation in DR prevalence according to the treatment method used to control diabetes. DR prevalence fell from 67.6% in participants who used insulin to 29.9% in participants who used oral medications without insulin to 7.5% in those who did not use medications. Duration of diabetes diagnosis and level of glycaemic control are both likely to be important confounding variables when examining treatment method. Unfortunately, we do not have the statistical power to examine treatment method with adjustment for duration and control.
Our study did not find any significant association between DR and age, ethnicity, BMI, glaucoma, myopia, or intake of aspirin, alcohol, or tobacco. The ETDRS randomised participants to either placebo or aspirin and showed no effect of aspirin on the course of retinopathy.25 The other variables listed have all been implicated as possibly being associated with DR but their significance remains unconfirmed.3 18 26 The relatively small number of people with DR in our population based study does not give us the statistical power to identify weak associations.
It is a concern that only about half of people with diagnosed diabetes have had a retinal examination in the previous 2 years as recommended by the National Health and Medical Research Council clinical practice guidelines.27 We found previously that 34% of people without DR and 25% of people with DR in Melbourne had never seen an ophthalmologist.28 We also found that although the majority of general practitioners report that they do not perform dilated funduscopy, they usually refer their patients with diabetes to an ophthalmologist.29 Currently, a national diabetes strategy is being implemented in Australia.30 One of its aims is to reduce complications in people with diabetes, including diabetic retinopathy. A measure of the success of this implementation strategy will be an increase in the percentage of people with diabetes who have the recommended 2 yearly dilated fundus examination.
Currently, there are only two available methods for preventing blindness from retinopathy in people with diabetes. Firstly, glycaemic control should be kept as strict as possible so that the development and progression of retinopathy can be delayed. Blindness prevention should be discussed along with treatment of hypertension and hyperlipidaemia with patients as the strongest incentives to achieve strict control. Secondly, regular screening of people with diabetes is required to identify vision threatening retinopathy as early as possible so that timely laser treatment can be given. In Victoria, we have identified that there is a small but important number of people in the community with known diabetes who have untreated, vision threatening retinopathy. The necessity of regular screening must be emphasised to all people with diabetes so that this number is kept to an absolute minimum.
Acknowledgments
The Visual Impairment Project is supported by the Victorian Health Promotion Foundation (Vic Health), The Ansell Ophthalmology Foundation, The National Health and Medical Research Council Sir John Eccles award to Professor HR Taylor, the estate of the late Dorothy Edols, and the Jack Brockhoff Foundation. Dr McCarty is the recipient of the Wagstaff fellowship in ophthalmology from the Royal Victorian Eye and Ear Hospital.