Comparative safety and effectiveness of sitagliptin in patients with type 2 diabetes: retrospective population based cohort study
BMJ 2013; 346 doi: https://doi.org/10.1136/bmj.f2267 (Published 25 April 2013) Cite this as: BMJ 2013;346:f2267
- D T Eurich, associate professor12,
- S Simpson, associate professor23,
- A Senthilselvan, professor1,
- C V Asche, director45,
- J K Sandhu-Minhas, research associate2,
- F A McAlister, professor67
- 1Department of Public Health Sciences, School of Public Health, University of Alberta, Edmonton, AB, Canada, T6G 2G3
- 2Alliance for Canadian Health Outcomes Research in Diabetes, University of Alberta, Edmonton, AB, Canada, T6G 2E1
- 3Faculty of Pharmacy and Pharmaceutical Sciences, University of Alberta, Edmonton, AB, Canada, T6G 2B7
- 4Center for Health Outcomes, University of Illinois College of Medicine at Peoria, Peoria, IL, 61656-1649, USA
- 5Department of Pharmacy Administration, University of Illinois at Chicago College of Pharmacy, Chicago, IL, 60612-7231, USA
- 6Department of Medicine, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, AB, Canada, T6G 2B7
- 7Patient Health Outcomes Research and Clinical Effectiveness, University of Alberta, Edmonton, AB, Canada, T6G 2B7
- Correspondence to: D T Eurich 2-040 Li Ka Shing Center for Health Research Innovation, University of Alberta, Edmonton, AB, Canada, T6G 2E1 deurich{at}ualberta.ca
- Accepted 27 March 2013
Abstract
Objective To determine if the use of sitagliptin in newly treated patients with type 2 diabetes is associated with any changes in clinical outcomes.
Design Retrospective population based cohort study.
Setting Large national commercially insured US claims and integrated laboratory database.
Participants Inception cohort of new users of oral antidiabetic drugs between 2004 and 2009 followed until death, termination of medical insurance, or December 31 2010.
Main outcome measure Composite endpoint of all cause hospital admission and all cause mortality, assessed with time varying Cox proportional hazards regression after adjustment for demographics, clinical and laboratory data, pharmacy claims data, healthcare use, and time varying propensity scores.
Results The cohort included 72 738 new users of oral antidiabetic drugs (8032 (11%) used sitagliptin; 7293 (91%) were taking it in combination with other agents) followed for a total of 182 409 patient years. The mean age was 52 (SD 9) years, 54% (39 573) were men, 11% (8111) had ischemic heart disease, and 9% (6378) had diabetes related complications at the time their first antidiabetic drug was prescribed. 14 215 (20%) patients met the combined endpoint. Sitagliptin users showed similar rates of all cause hospital admission or mortality to patients not using sitagliptin (adjusted hazard ratio 0.98, 95% confidence interval 0.91 to 1.06), including patients with a history of ischemic heart disease (adjusted hazard ratio 1.10, 0.94 to 1.28) and those with estimated glomerular filtration rate below 60 mL/min (1.11, 0.88 to 1.41).
Conclusions Sitagliptin use was not associated with an excess risk of all cause hospital admission or death compared with other glucose lowering agents among newly treated patients with type 2 diabetes. Most patients prescribed sitagliptin in this cohort were concordant with clinical practice guidelines, in that it was used as add-on treatment.
Introduction
Glycemic control is considered one of the cornerstones in the management of type 2 diabetes. In addition to lifestyle changes, most patients will need glucose lowering treatment; most international guidelines recommend metformin as first line treatment.1 2 3 Over the past few years, several new treatments have been introduced, most notably the new class of oral “incretin” drugs known as the dipeptidyl peptidase-4 (DPP-4) inhibitors. The DDP-4 inhibitors lower blood glucose by inactivating DPP-4, an enzyme responsible for metabolizing the gastrointestinal hormone glucagon-like peptide-1, which is responsible for augmenting the release of insulin in response to a rise in blood glucose.
Sitagliptin was the first DPP-4 inhibitor based treatment to be marketed in the United States in 2007, followed by saxagliptin in 2009. DPP-4 inhibitors are considered weight neutral and have been shown to modestly improve modulators of cardiovascular risk, including triglycerides, low density lipoprotein cholesterol, high density lipoprotein cholesterol, and blood pressure; however, the data are relatively inconsistent across studies.4 5 6 Several pooled safety analyses have suggested potential benefits associated with DPP-4 inhibitors. A recent meta-analysis of 18 phase III randomized controlled trials reported that DDP-4 inhibitors were associated with a 52% (95% confidence interval 0.31% to 0.75%) relative risk reduction in major adverse cardiovascular events (cardiovascular death, non-fatal myocardial infarction or acute coronary syndrome, stroke, arrhythmias, and heart failure) compared with other active or placebo treatment.7 However, no evaluation of broader outcomes of interest to clinicians such as all cause death or all cause hospital admissions were reported. To date, evidence on the potential benefits or risks of DPP-4 inhibitors is lacking, and, given recent experiences with other novel glucose lowering treatments such as thiazolidinediones, concerns exist.8 9
Although several studies assessing specific safety endpoints (pancreatitis, upper respiratory tract infections, renal failure) have been done,10 11 12 13 to our knowledge no large comparative effectiveness studies have evaluated sitagliptin, the most widely prescribed and longest marketed DPP-4 inhibitor in the United States, in “real world” patients with broader outcomes including all cause hospital admissions or mortality. We thus designed this study to compare outcomes associated with sitagliptin treatment compared with other glucose lowering agents. We hypothesized that the use of sitagliptin would not be associated with increased risk of hospital admission, mortality, or cardiovascular events.
Methods
We did a population based retrospective cohort study using a large US claims and integrated laboratory database that included employed, commercially insured patients with dependants from all 50 states (Clinformatics Data Mart, OptumInsight Life Sciences Inc). Patient level data are collected directly from the clinical encounter, providing a unique, clinically rich source of information. The database has been widely used and includes de-identified longitudinal data on patients, including administrative and demographic data (type of insurance plan, sex, age, dates of eligibility, income) and all billable medical service claims including inpatient and outpatient visits and medical procedures (de-identified physician and facility identifier, date and place of service, cost of service, admission and discharge dates, procedure and diagnosis codes), all laboratory tests and results (lipids (high density lipoprotein cholesterol, low density lipoprotein cholesterol, triglycerides), renal function (creatinine, proteinuria), liver function, blood glucose (glycated hemoglobin), complete blood count, and so on), and pharmacy claims data (de-identified prescribing physician, drug dispensed based on national drug codes, quantity and date dispensed, drug strength, days’ supply, cost of service).14 15 16 17 All clinical diagnoses are recorded according to ICD-9-CM (international classification of diseases, 9th revision, clinical modification) codes and procedure codes (according to ICD-9 and current procedural terminology 4 codes). The database contains more than 13 million annual lives, and data are updated every 90 days. We de-identified and accessed the data by using protocols compliant with the Health Insurance Portability and Accountability Act.
Cohort selection
We identified an inception cohort of new users of oral antidiabetic drugs between the index years of January 1 2004 and December 31 2009. We defined new users as those with no prescription records for any antidiabetic drug, including insulin, for one year before their index date (that is, the date of the first claim for their antidiabetic drug).18 19 20 To be included, all patients had to be at least 20 years of age on the index date, be enrolled in a commercial medical insurance plan, and have one year of continuous medical insurance before the index date (fig 1⇓). We excluded patients starting insulin as their first antidiabetic agent, but progression from oral antidiabetic treatment to insulin was allowed during follow-up. We subsequently followed all patients until death, termination of medical insurance, or December 31 2010, providing a maximum follow-up of six years. As saxagliptin was released only in July 2009, and few patients were using it in our inception cohort (n=610), we excluded these patients from our primary analysis, although we included them in a sensitivity analysis.

{kind=link}
Our primary outcome was all cause hospital admission or death. We also analyzed each component of the composite endpoint (all cause death or all cause hospital admission) separately. In addition, we evaluated the effect of sitagliptin on cardiovascular related hospital admissions (ICD-9-CM codes 410, 411.1, 428, 430-438) and the combined endpoint of cardiovascular related hospital admission or all cause mortality. For the composite outcomes, we used time to the first event (either admission date or date of death) as the dependent variable (failure time) in our main analysis. Patients who did not reach the outcome of interest were censored at their study exit date. We ascertained vital status through linkage to the US national death index file.21 This is considered to be highly valid and reliable for matching of death, with greater than 98% sensitivity when social security number data are available, as in our case.22 We did not have access to cause of death in the data.
Analysis
As the patterns of glucose lowering treatment are quite complex, we used time varying Cox proportional hazards regression to estimate more precisely the effect of exposure to drug. In these analyses, we set time zero at the start of the first oral antidiabetic drug use.23 We established time varying exposure to oral antidiabetic drugs and insulin on the basis of the expected duration of each prescription by using the “days’ supplied” field in the prescription drug dispensations database.24 We considered patients to be exposed to the drug of interest unless they did not refill their prescription for two consecutive periods (based on the days’ supply field) of the previous prescription. We then considered patients as unexposed to the drug of interest for the period of time from the end of the first consecutive period to the end of the study or until they restarted the drug. Subsequent definitions whereby we considered participants as non-exposed immediately after the expected duration and definitions that allowed for a 14 day “grace period”24 did not appreciably change our results and are otherwise not presented. We attributed outcome events to the drugs the patient was expected to be receiving at the time of the event, and we assumed no legacy or carryover effects from remote exposure to any of the glucose lowering drugs for the primary analysis, although we assessed legacy effects in sensitivity analyses.
Exposure to antidiabetic drugs
For the primary exposure of interest, for each day of follow-up, we classified exposure to antidiabetic drugs into six categories that were not mutually exclusive: any sitagliptin use, any metformin use, any sulfonylurea use, any thiazolidinedione use, other oral antidiabetic drug use (acarbose, meglitinides, pramlintide), and any insulin use. For analyses, we included each drug exposure class in the model as a dummy variable with the reference group being no exposure to the drug of interest (for example, exposure to sitagliptin compared with no exposure to sitagliptin, after adjustment for use/non-use of other antidiabetic drugs). We classified patients receiving combination pills (such as sitagliptin and metformin) as receiving both agents concurrently (that is, any sitagliptin use and any metformin use). In addition, we specifically evaluated the potential effects of sitagliptin in subgroups at high risk, such as those with a history of ischemic heart disease or those with estimated glomerular filtration rate below 60 mL/min at the index date. Secondarily, as current clinical practice guidelines recommend that sitagliptin should be used as add-on treatment,1 3 we specifically evaluated the effects of sitagliptin used in combination. Thus, we further classified drug exposure into mutually exclusive categories of combination treatment and included this variable in our model as our exposure of interest: sitagliptin plus metformin, sitagliptin plus a sulfonylurea, and metformin plus a sulfonylurea. For these analyses, the metformin plus sulfonylurea combination treatment group served as our reference category (usual guideline recommended care).1 3
Confounding variables
In addition to the time varying exposure to oral antidiabetic drugs and insulin, we included numerous additional confounding variables in the Cox regression models as time fixed variables in the analyses on the basis of the most recent value within one year before starting glucose lowering treatment, as sitagliptin has been shown to alter several potential risk factors.5 The specific variables included were age, sex, socioeconomic status (type of medical insurance and median household income according to the 2010 US census25), clinical laboratory data (glycated hemoglobin, high density lipoprotein cholesterol, low density lipoprotein cholesterol, triglycerides, estimated glomerular filtration rate (according to the modified diet in renal disease calculation: ≥90, 89.9-60, 59.9-30, <30 mL/min), albuminuria, hemoglobin concentrations), and prescription drugs (for example, antiplatelet drugs, anticoagulants, statins, calcium channel blockers, β blockers, angiotensin converting enzyme inhibitors/angiotensin receptor blocker, renin inhibitors, diuretics, nitrates). For patients who did not have specific clinical laboratory data measured, we used the missing indicator approach for all analyses.26 To further control for comorbidities, we used the adjusted clinical groups score derived from the Johns Hopkins ACG system, version 9,27 which is a single comorbidity score weighted by the 32 adjusted diagnostic groups that performs equally to or better than the Charlson and Elixhauser comorbidity scores.28 In addition, we included the expanded diagnosis cluster for diabetes to further control for diabetes specific complications.27 We also included adherence to glucose lowering treatments in our models by using the medication possession ratio based on the prescription days’ supply field.
To further control for confounding by indication, we used several techniques. Firstly, as we have previously done,29 assuming that sicker patients are more likely to be admitted to hospital, we included the total number of hospital admissions in the year before the index date as a covariate in analyses. Secondly, from the Johns Hopkins ACG system, we included the total number of chronic conditions identified as a marker of global comorbidity, as well as a medically frail condition marker as derived by the system (for example, any occurrence of malnutrition, abnormal weight loss, morbid obesity, dementia, falls, decubitus ulcer).27 Lastly, as others have, we included a time varying propensity score whereby we updated the propensity or probability of receiving sitagliptin every three months throughout the follow-up period by using all available data to date.30 The propensity score contained almost 60 variables, including demographic variables (age, sex, age-sex interaction, state, type of insurance), socioeconomic factors (income), comorbidities, health service use, laboratory data, markers of frailty, and drug treatments. We observed no clinically important differences in covariates within fifths of the propensity score between patients exposed to sitagliptin and those not exposed. For example, for patients in the highest propensity fifth, background use of both metformin (82% v 83%) and sulfonylureas (32% v 31%) was very similar for sitagliptin users and non-users.
Sensitivity analyses
To evaluate the robustness of our results, we did several additional analyses. Firstly, as sitagliptin was not available until 2007, we restricted our new user cohort to the years of 2007-09. Secondly, we excluded all patients using insulin treatment, as insulin may be viewed as a marker for more advanced disease, and repeated our analyses. Thirdly, we modified our definition of exposure whereby we considered patients as unexposed to the drug of interest for all future periods if they stopped using the drug for at least two consecutive periods (that is, restarting of drugs was not allowed). Fourthly, we evaluated any “legacy” effects by considering patients as exposed in all future time periods if they had any previous exposure to the drug of interest. Fifthly, we censored patients if they stopped all antidiabetic drugs (including insulin) for at least two consecutive periods. Sixthly, we combined sitagliptin use with users of saxagliptin (n=610) to evaluate the overall effect of DDP-4 inhibitors. Seventhly, we evaluated the association between sitagliptin use and acute pancreatitis or upper respiratory tract infections, which have been reported in the literature.10 11 13 Lastly, we repeated our main analyses using a high dimensional propensity score that uses an algorithm to empirically identify candidate covariates. This method creates and prioritizes potential confounders by using all available diagnostic codes, procedural codes, hospital admissions, drugs, and laboratory values. From this exhaustive list, the top 500 most influential covariates on the association of interest are selected to generate the propensity score. Use of the high dimensional propensity score has been shown to improve effect estimates compared with predefined covariate based propensity scores.31
Results
Between 2004 and 2009, 72 738 new users of oral antidiabetic drugs met the inclusion and exclusion criteria (fig 1⇑). The average age was 52 (SD 9) years, 54% were men, 10% had a history of ischemic heart disease, and 9% had diabetes related complications (table 1⇓). We identified 8032 (11%) patients who used sitagliptin at any point during the study. Although statistical differences existed between sitagliptin and non-sitagliptin users owing to the large numbers, few clinically important differences existed with the exception that sitagliptin users tended to have higher use of insulin treatment and higher rates of diabetes related complications (table 1⇓). Among sitagliptin users, most (7293; 91%) used sitagliptin as an add-on treatment with other oral agents, consistent with current clinical practice guidelines.
Baseline characteristics according to drug use at any time during follow-up. Values are numbers (percentages) unless stated otherwise
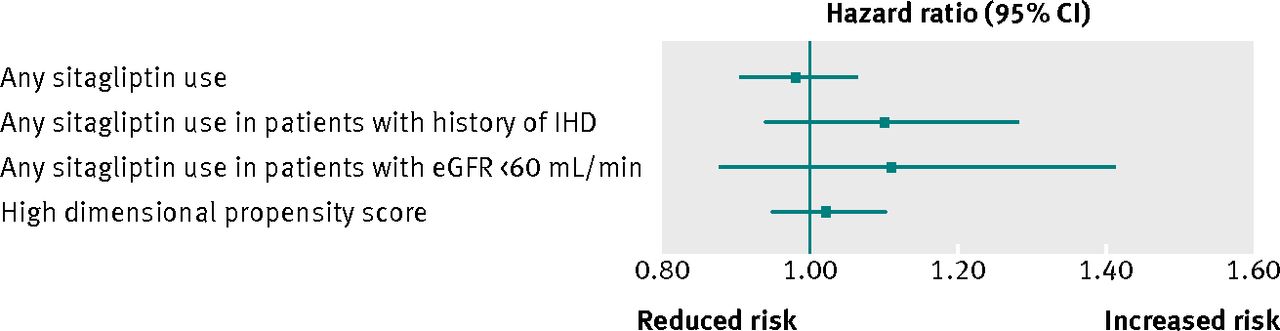
By the end of follow-up (182 409 patient years with a mean duration of 2.5 (SD 1.7) years), our primary composite endpoint had occurred in 14 215 (20%) patients: 14 121 (19%) patients were admitted to hospital at least once, and 520 (1%) died (table 2⇓). Users of sitagliptin had lower crude incident rates of all cause hospital admission or all cause mortality compared with other antidiabetic agents. However, in time varying multivariable Cox regression analysis, sitagliptin users had similar hazards for the primary composite endpoint to sitagliptin non-users after adjustment for the use of other glucose lowering strategies, demographics, and clinical and comorbidity data (adjusted hazard ratio 0.98, 95% confidence interval 0.91 to 1.06) (table 2⇓). Similarly, sitagliptin users had a similar risk to non-users for the combined endpoint of cardiovascular related hospital admissions or all cause mortality (adjusted hazard ratio 0.92, 0.79 to 1.07), all cause mortality (1.14, 0.79 to 1.65), all cause hospital admissions (0.98, 0.91 to 1.06), and cardiovascular related hospital admissions (0.90, 0.77 to 1.07) (table 2⇓; fig 2⇓).
Outcomes according to antidiabetic drug exposure

Fig 2 Adjusted hazard ratios and 95% confidence intervals for the outcome of all cause hospital admission or all cause death according to sitagliptin exposure (compared with no sitagliptin use in time varying Cox proportional hazards analysis adjusted for covariates in footnote to table 2). eGFR=estimated glomerular filtration rate; IHD=ischemic heart disease
{kind=link}
Among patients with a history of ischemic heart disease, sitagliptin users had a similar risk to non-users for the primary composite endpoint (adjusted hazard ratio 1.10, 0.94 to 1.28), the combined endpoint of cardiovascular related hospital admissions or mortality (0.99, 0.77 to 1.27), all cause mortality (1.02, 0.53 to 1.99), all cause hospital admissions (1.10, 0.94 to 1.28), and cardiovascular related hospital admissions (0.98, 0.76 to 1.27). Similarly, in those with estimated glomerular filtration rate below 60 mL/min, sitagliptin users had a similar risk to non-users for the primary composite endpoint (adjusted hazard ratio 1.11, 0.88 to 1.41), the combined endpoint of cardiovascular related hospital admissions or mortality (0.86, 0.34 to 1.37), all cause mortality (0.99, 0.34 to 2.89), all cause hospital admissions (1.10, 0.87 to 1.40), and cardiovascular related hospital admissions (0.92, 0.57 to 1.50) (fig 2⇑).
Compared with users of metformin plus a sulfonylurea, users of sitagliptin plus a sulfonylurea had a similar risk for our primary composite endpoint (adjusted hazard ratio 1.03, 0.76 to 1.39), whereas use of sitagliptin plus metformin was associated with lower risk (0.82, 0.72 to 0.93). Subsequent post hoc analyses in which we restricted our entire cohort to only new users of metformin (n=55 678), which is recommended first line treatment for most patients with type 2 diabetes, confirmed these results: adjusted hazard ratio 0.85, 0.74 to 0.98 for addition of sitagliptin to metformin compared with addition of a sulfonylurea to metformin. However, an analysis of only new users of sulfonylureas as first line treatment did not show any difference between those patients who switched to sitagliptin plus metformin and users of sulfonylurea who added metformin (adjusted hazard ratio 1.04, 0.71 to 1.53).
Restriction of cohort entry to begin in 2007 did not materially change our results for sitagliptin use compared with non-use for the primary combined endpoint (adjusted hazard ratio 1.00, 0.91 to 1.10). Analyses excluding insulin users produced nearly identical results to our main findings on use of sitagliptin for the composite endpoint (adjusted hazard ratio 1.01, 0.94 to 1.09). Our results were also robust to changes in the definition of exposure whereby we considered patients as unexposed if they stopped the drug of interest for at least two consecutive periods (that is, no restarts allowed) (adjusted hazard ratio 0.97, 0.90 to 1.05), as they were to consideration of a legacy effect of any previous exposure (0.97, 0.91 to 1.04) and censoring of patients after they discontinued all drugs, including insulin, for at least two consecutive periods (0.99, 0.91 to 1.06). The inclusion of the 610 patients using saxagliptin provided nearly identical results to those observed with sitagliptin alone (adjusted hazard ratio 0.98, 0.91 to 1.05). We also found no association between the use of sitagliptin and the risk of acute pancreatitis (adjusted hazard ratio 1.10, 0.68 to 1.77) or the risk of acute upper respiratory tract infections (P=0.97) or pancreatic cancers (P=0.96) compared with sitagliptin non-users. Finally, the inclusion of a high dimensional propensity score did not change any of our estimates materially (adjusted hazard ratio 1.02, 0.95 to 1.10 for sitagliptin users compared with sitagliptin non-users for the primary combined endpoint).
Discussion
In our large clinically rich population, we found that the use of sitagliptin was not associated with any appreciable excess risk of all cause hospital admission or all cause mortality in a broad spectrum of patients with newly treated diabetes or in higher risk groups such as those with a history of ischemic heart disease or with reduced kidney function. Importantly, we also did not observe any safety “signals” related to cardiovascular related hospital admissions or death, supporting the premise that sitagliptin seems to be safe in patients with diabetes, at least if used in the manner in which it was used in this cohort. To our knowledge, this is the first study to evaluate the comparative effectiveness and safety of sitagliptin, or any of the DPP-4 inhibitors, at the population level. Given the current controversy about other antidiabetic agents, most notably the thiazolidinediones, this is important information for patients and for clinicians managing blood glucose concentrations in patients with diabetes.
Comparison with other studies
Although this is the first population based study assessing the effect of DPP-4 inhibitors on mortality and cardiovascular events, our results are broadly consistent with previous observational studies that have shown that sitagliptin is not associated with an increased risk of acute pancreatitis10 11; however, unlike previous studies,13 we did not find any association with upper respiratory tract infections, although previous estimates of upper respiratory tract infections may have substantial reporting bias.13 Our results are not consistent with recent meta-analyses of published and unpublished randomized controlled trials reporting that various DDP-4 inhibitors (alogliptin, dutogliptin, linagliptin, saxagliptin, sitagliptin, and vildagliptin) are associated with statistically significant 30-60% reductions in major adverse cardiac events and non-significant 33% and 48% reductions in all cause and cardiovascular death compared with other active drugs or placebo treatment.7 32 33 Importantly, these analyses included studies of relatively short duration and that enrolled highly selected patients. Although modulation of the glucagon-like peptide-1 system has been shown to have pleiotropic effects on the cardiovascular system,6 34 we did not observe any significant benefits, or risk, at the population level. However, our analyses also suggest that sitagliptin was prescribed in our cohort for patients with more advanced diabetes, given the higher rates of complications of diabetes at baseline and higher glycated hemoglobin values. Thus, despite the use of time varying propensity scores, any potential beneficial effects of sitagliptin on morbidity and mortality may have been masked by the higher baseline risk of patients prescribed sitagliptin in our cohort.
Combination treatment
Our results also suggest that differences may exist between the use of sitagliptin in combination with metformin and the use of sitagliptin in combination with sulfonylureas. Whether this effect is truly related to the use of sitagliptin as opposed to a metformin effect is uncertain. A large body of observational data on the use of metformin has consistently shown that users of metformin have lower morbidity and mortality rates than sulfonylurea users.19 20 35 36 However, in our cohort, metformin users tended to have better glycemic control at baseline and less comorbidity and were less likely to use additional treatment, so our results may simply represent residual confounding. On the other hand, we found that those metformin treated patients prescribed sitagliptin as add-on treatment had better outcomes than those prescribed a sulfonylurea as add-on treatment. As metformin is recommended first line treatment for most patients with type 2 diabetes, our results may have important implications for the selection of add-on treatment in these patients. However, we acknowledge that these analyses were post hoc and exploratory in nature and should be considered hypothesis generating rather than definitive.
Strengths and limitations of study
Despite several strengths of our study, including the availability of detailed clinical data (such as glycated hemoglobin, cholesterol, and markers of renal function), the use of advanced statistical techniques including time varying propensity scores, and the relatively large sample size of new users of antidiabetic agents, several limitations are inherent to our work. Firstly, and most importantly, this is an observational study and any results must be interpreted with caution. Our results may be attributed to selection bias in that physicians may have given or withheld sitagliptin in patients perceived to be at varying degrees of risk, which even time varying propensity scores cannot fully adjust for. Secondly, we were not able to fully adjust for unmeasured confounders such as blood pressure or body weight. For example, sitagliptin may have been reserved for heavier patients because of its neutral effect on weight gain. However, this selection bias would actually strengthen our conclusions on the safety of sitagliptin, as it would have biased towards higher event rates in sitagliptin users; thus, if anything, our results would have underestimated any potential benefits of sitagliptin on morbidity or mortality. Moreover, although we did not have actual blood pressure measurements, we did include physician assigned diagnosis of hypertension or related comorbidities, as well as all major blood pressure lowering drug classes, in both our propensity score and adjusted analyses. A third limitation is that our population largely consisted of middle aged patients with commercial health insurance. Fourthly, as DPP-4 inhibitors have only recently been marketed, our study had a relatively short follow-up duration (mean 2.5 years). Although no short term adverse events were noted with sitagliptin, the longer term safety of sitagliptin cannot be fully elucidated yet. Finally, we did not have data on other potential adverse outcomes not requiring admission to hospital and thus cannot comment on the safety of sitagliptin with respect to these endpoints.
Conclusions
Our results suggest that clinicians have rapidly adopted the use of sitagliptin in the management of type 2 diabetes, but in most cases it is being used as add-on treatment rather than initial monotherapy (congruent with guidelines during the time of our study).1 2 3 Initial evidence from phase III clinical trials and pre-clinical data suggest cardiac benefits with DPP-4 inhibitors, but we did not observe any clinically important effects in newly treated patients with type 2 diabetes. Although results of the ongoing Trial Evaluating Cardiovascular Outcomes With Sitagliptin (TECOS) are needed to definitively assess the safety of sitagliptin in patients with diabetes and cardiovascular disease, the trial is not scheduled to report for several years and will not cover the comparative effectiveness and safety of sitagliptin in the broader population with diabetes. Until then, our observational data provide evidence of the comparative effectiveness and safety of this agent and support the recommendations in current clinical practice guidelines to use sitagliptin as needed in people with diabetes.1 3
What is already known on this topic
Several pooled safety analyses have suggested potential benefits associated with dipeptidyl peptidase-4 inhibitors
No large published studies have evaluated the effect of sitagliptin on broad outcomes such as all cause hospital admissions or mortality in “real world” patients
What this study adds
Sitagliptin was not associated with any appreciable excess risk of all cause hospital admission or all cause mortality in a broad spectrum of patients with newly treated diabetes
Nor was it associated with excess risk in higher risk groups such as patients with a history of ischemic heart disease or with reduced kidney function
These observational data provide evidence of the comparative safety of sitagliptin and support current recommendations to use sitagliptin as add-on treatment if needed in people with diabetes
Notes
Cite this as: BMJ 2013;346:f2267
Footnotes
We acknowledge the tremendous support from Betsey Jackson at Health Data Services Corporation (www.hdscorp.biz), P O Box 53, Carlisle, MA 01741, USA, for providing independent database acquisition services.
Contributors: All authors contributed to the conception and design of the study. DTE, JKS-M, AS, SS, and FAM contributed to the analysis and interpretation of data. DTE and JKS-M drafted the article, all authors revised it critically for important intellectual content, and all authors provided final approval of the version to be published. DTE is the guarantor.
Funding: This work was funded by operating grants from the Canadian Diabetes Association (OG-2-09-2691-DE) and the Canadian Institutes of Health Research (CIHR) (MOP-126093). DTE receives salary support from Alberta Innovates Health Solution (AIHS) and the CIHR. FAM is a senior health scholar with AIHS. The study sponsors played no role in study design or conduct; collection, analysis, or interpretation of data; writing of the report; or the decision to submit the paper for publication.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: The study was approved by the ethics review board of the University of Alberta, Edmonton, Alberta, Canada, and the New England Institutional Review Board, United States.
Data sharing: No additional data available.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/.