Incidence of type 1 diabetes in China, 2010-13: population based study
BMJ 2018; 360 doi: https://doi.org/10.1136/bmj.j5295 (Published 04 January 2018) Cite this as: BMJ 2018;360:j5295
- Jianping Weng,
- Zhiguang Zhou,
- Lixin Guo,
- Dalong Zhu,
- Linong Ji,
- Xiaoping Luo,
- Yiming Mu,
- Weiping Jia
- on behalf of the T1D China Study Group
- Correspondence to: J Weng, Department of Endocrinology and Metabolic Disease, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou 510630, China wjianp{at}mail.sysu.edu.cn
- Accepted 31 October 2017
Abstract
Objective To estimate the incidence of type 1 diabetes in all age groups in China during 2010-13.
Design Population based, registry study using data from multiple independent sources.
Setting National registration system in all 505 hospitals providing diabetes care, and communities of patients with diabetes in 13 areas across China, covering more than 133 million person years at risk, approximately 10% of the whole population.
Participants 5018 people of all ages with newly diagnosed type 1 diabetes and resident in the study areas from 1 January 2010 to 31 December 2013.
Main outcome measures Incidence of type 1 diabetes per 100 000 person years by age, sex, and study area. Type 1 diabetes was doctor diagnosed and further validated by onsite follow-up. Completeness of case ascertainment was assessed using the capture mark recapture method.
Results 5018 cases of newly diagnosed type 1 diabetes were ascertained: 1239 participants were aged <15 years, 1799 were aged 15-29 years, and 1980 were aged ≥30 years. The proportion of new onset cases in participants aged ≥20 years was 65.3%. The estimated incidence of type 1 diabetes per 100 000 persons years for all ages in China was 1.01 (95% confidence interval 0.18 to 1.84). Incidence per 100 000 persons years by age group was 1.93 (0.83 to 3.03) for 0-14 years, 1.28 (0.45 to 2.11) for 15-29 years, and 0.69 (0.00 to 1.51) for ≥30 years, with a peak in age group 10-14 years. The incidence in under 15s was positively correlated with latitude (r=0.88, P<0.001), although this association was not observed in age groups 15-29 years or ≥30 years.
Conclusion Most cases of new onset type 1 diabetes in China occurred among adults. The incidence of type 1 diabetes in Chinese children was among the lowest reported in the study.
Introduction
International studies of type 1 diabetes ,12 such as the DiaMond (Diabetes Mondiale) Project and European Community Concerted Action Programme in Diabetes (EURODIAB) study have shown wide variation in the incidence of type 1 diabetes among children. According to the DiaMond Project, China had one of the lowest incidences of type 1 diabetes in children—0.51 per 100 000 person years during 1985-94.3 A nationwide registry of type 1 diabetes in China does not exist.
The incidence of type 1 diabetes in children has been increasing worldwide.245 Recent results of the SEARCH for Diabetes in Youth study from the United States suggest that environmental or behavioural factors, or both, play larger parts in the increased incidence of type 1 diabetes compared with decades ago.56 The study of type 1 diabetes in a low incidence region such as China may help advance the understanding of the contribution of varying combinations of genetic and environmental factors to the development of the disease. Moreover, most epidemiological studies of type 1 diabetes focused on childhood onset type 1 diabetes. Although type 1 diabetes most often develops in children, it can occur at any age.78 Our previous study also indicated that the onset of type 1 diabetes in adulthood is not rare in China.9 Yet little is known about its incidence in adults aged more than 20 years.10
We carried out a nationwide, population based registry study (the Epidemiological Study of Type 1 Diabetes Mellitus in China (T1D China)) to investigate the incidence of type 1 diabetes in all age groups in China during 2010-13.
Methods
Our study is a population based multicentre observational study, with ascertainment of doctor diagnosed cases of type 1 diabetes. We identified new cases occurring during 2010 to 2013 in the resident population of 13 areas across China (Harbin, Shenyang, Beijing, Shanghai, Nanjing, Jinan, Wuhan, Changsha, Guangzhou, Chengdu, Xi’an, Lanzhou, Yinchuan; fig 1, and see supplementary table S1).

Thirteen study areas in China, 2010-13. The study was conducted in mainland China. Hong Kong and Macao not included
Study population
Our study population comprised residents of 13 study areas. These areas were chosen from the seven administrative regions of China (northeast, north, northwest, southwest, central, east, and south) according to geographical location, climate, culture, ethnicity, and population, and they are representative of the seven administrative regions. We selected at least one area from each of these administrative regions. Besides, a huge imbalance in population density exists in China: more than 90% of the population reside in the southeast. We also ensured that there was at least one study area every 5° of latitude (fig 1, and see supplementary table S1). In some of the administrative regions we therefore selected one or two additional areas. The study areas also consist of regions of different economic development levels, as represented by the gross domestic product in 2010.11 The study areas covered the less developed, moderately developed, and well developed areas in China.
The study population (denominator) included residents of all ages in the 13 study areas during 2010 to 2013. According to the 2010 Chinese census,12 we defined the resident population as: people whose registered address agreed with their primary address and who had stayed at their primary address for six months or more; people whose registered address disagreed with their primary address, but who had stayed at their primary address for six months or more; people whose registered address disagreed with their primary address, but who had stayed at their primary address for less than six months; and people in active military service and those whose primary address could not be specified—they were not included in the resident population.
The 2010 Chinese census12 conducted by the National Bureau of Statistics of China provides precise information on China’s mainland population, which is essential for the calculation of the denominator in a nationwide registry study. Our study period was 1 January 2010 to 31 December 2013, which allowed at least 18 months of a diagnostic time window for cases to be included in our study when we started the onsite data validation and inspection (see supplementary materials, section 4) in June 2015. We estimated the denominator yearly according to the 2010 Chinese census and annual government reports on natural population growth (see supplementary materials, section 2). Derivation of appropriate denominators is a multistep process, adjusted for sex categorisation and the natural growth rate of the local population. Our study population covered more than 133 million person years at risk between 2010 and 2013, which represents approximately 10% of the Chinese population, including 6% of those aged less than 15 years. This provided enough power to estimate the incidence over 1.0 per 100 000 person years.
The numerator included all newly diagnosed cases of type 1 diabetes in the resident population in the study areas from 1 January 2010 to 31 December 2013.
Data sources and collection
The data coordinating service provider collected and submitted data from four sources: the medical record databases from all the hospitals providing diabetes care in the 13 study areas (505 hospitals); outpatient based pharmacies in tertiary hospitals in the 13 areas (228 hospitals); government medical insurance databases; and patient self reports from online and offline communities of patients with diabetes spontaneously founded and maintained by patients with diabetes or their family members, or both, which were confirmed by medical records (see supplementary materials, section 2).
Collected data included identification markers and clinical information. Identification markers included mandatory and optional markers. For all validated cases, mandatory markers, including initials of each Chinese character of the name, sex, date of birth, registered address, primary address, date of diabetes diagnosis, date of insulin treatment initiation, hospitals where treated (with inpatient or outpatient status, or both, specified), and ethnicity, were collected, usually as part of the case validation process. For cases from communities of patients with diabetes, we collected mandatory information from the hospital where diabetes was first diagnosed. We excluded cases with missing mandatory information after onsite validation. Supplementary materials section 2 lists the optional markers. Clinical information was collected from medical record databases, as part of the case ascertainment process, including clinical presentations at onset (symptoms, occurrence of diabetic ketosis or ketoacidosis), family history, treatment for hyperglycaemia, C peptide level at onset or within 12 months after diagnosis, and presence of diabetes autoantibodies at any time.
The data coordinating service provider registered and anonymised the cases and sent the information to the data management committee. Mandatory information was available in 98.8% of cases. Data managers used identification markers for matching within the same source and across sources to identify potential duplicate records at area level (see supplementary materials, section 3, part 4)
Case ascertainment
Participating endocrinologists or paediatricians, or both, or an expert committee on type 1 diabetes established the diagnosis (see supplementary materials, section 1). The clinical diagnosis of type 1 diabetes was based on the American Diabetes Association descriptions of type 1 diabetes8 and the World Health Organization reports on the classification of diabetes.13 Diabetic ketoacidosis was defined based on guidelines1415 and data accessibility in China. Diabetic ketoacidosis was diagnosed in people with the following history and laboratory results: hyperglycaemia (glucose >11.1 mmol/L) or known diabetes ; ketonemia: raised levels of blood ketobodies as judged by participating investigators, or important ketonuria (>++ on standard urine dipsticks); and acidemia: bicarbonate (HCO3-) <15.0 mmol/L or venous pH <7.3, or both.
Data managers examined all submitted information to identify participants with an uncertain diagnosis of type 1 diabetes. Uncertain results were sent back to the data coordinating service provider. This provider required the corresponding investigator to feedback on the diagnosis of type 1 diabetes and provide any previously absent data related to the diagnosis if available. The corresponding investigator would make the judgment of diagnosis based on the currently available data, and would follow-up the patient if necessary and then give feedback to the data coordinating service provider. We ensured that the diagnostic time window would be no less than 18 months for participants, as a report shows that 18 months is the usual duration from the time a patient first sees a doctor to the final diagnosis.16 The data coordinating service provider informed the data managers of the feedback. Any cases of uncertain diagnosis were submitted to the expert committee for final judgment. We ascertained all cases with a final diagnosis of type 1 diabetes (see supplementary materials, section 3).
Statistical analysis
To assess the completeness of case ascertainment we used the capture mark recapture method17 and a two-mode ascertainment model (see supplementary materials, section 5). We defined the percentage of completeness of ascertainment for each study area as the number of observed cases divided by the number estimated from the capture mark recapture method. Incidence by age group, sex, and area were calculated per 100 000 person years at risk, and we calculated 95% confidence intervals based on inverting the score test for a binomial proportion.18 The model to estimate the national incidence of type 1 diabetes in China was developed from data collected in the 13 study areas and based on a Poisson distribution, in which factors potentially affecting the incidence of type 1 diabetes were added as covariates (see supplementary materials, section 6). Pearson’s χ2 analysis was applied to comparison of rates. Spearman correlation was used to analyse the relation between incidence and potentially related factors. For all statistical analyses we used SAS version 9.4 (SAS Institute, Cary, NC). We considered P<0.05 to be statistically significant.
Patient involvement
No patients were involved in setting the research question or the outcome measures, nor were they involved in developing plans for recruitment, design, or implementation of the study. No patients were asked to advise on interpretation or writing up of results. However, patient self reports were collected from online and offline communities of patients with diabetes spontaneously founded and maintained by patients with diabetes or their family members, or both. We contacted the founders and the people currently in charge of these communities and released a questionnaire asking for members of these communities to volunteer to self report. No patient or their family members were involved in the design of such a questionnaire, and the information collected from the questionnaire was anonymised. There are no plans to disseminate the results of the research to study participants.
Results
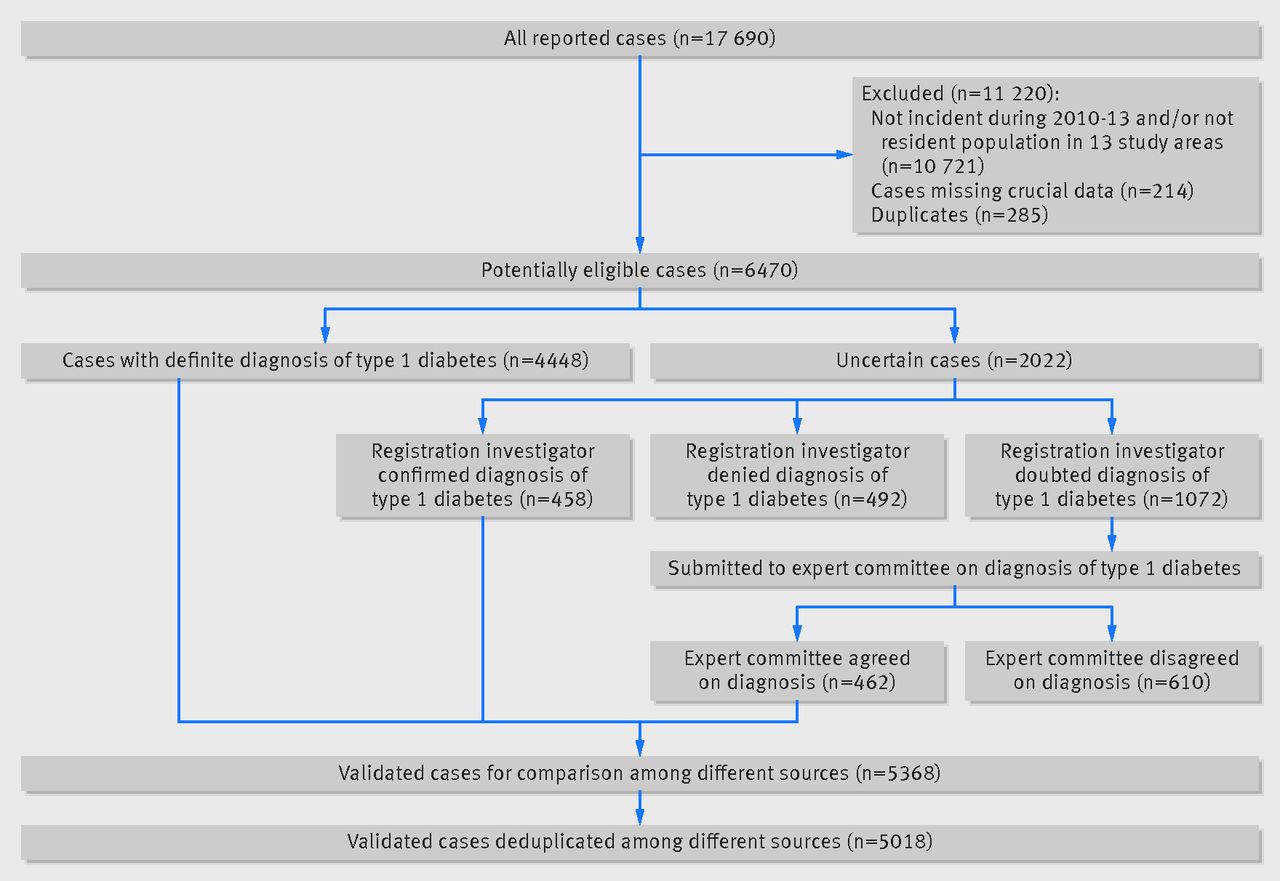
Our study population comprised 5018 people with type 1 diabetes newly diagnosed between 2010 and 2013 (fig 2): 1239 were aged 0-14 years, 1799 were aged 15-29 years, and 1980 were aged ≥30 years, and 2755 (54.9%) were male. Table 1 summarises the number of participants and the estimated annual incidence in each study area. Completeness of ascertainment was estimated to be more than 95% across the 13 areas. Completeness was relatively even among age groups, at 99.3% in the 0-14 years group, 98.4% in the 15-29 years group, and 98.8% in the ≥30 years group. (see supplementary table S3).

{kind=link}
{kind=link}
Incidence of type 1 diabetes in different age groups in 13 areas of China
After adjustment for the denominator of annual change in population between 2010 and 2013, the overall estimated incidence of type 1 diabetes per 100 000 person years for all ages in the 13 study areas was 0.93 (95% confidence interval 0.90 to 0.95). There was a slight difference (P<0.001, χ2=30.43) between males (0.95 per 100 000 person years, 0.91 to 0.99) and females (0.81 per 100 000 person years, 0.78 to 0.85; table 2). The incidence (per 100 000 person years) by age group was 1.90 (95% confidence interval 1.80 to 2.01) for 0-14 years, 1.02 (0.98 to 1.07) for 15-29 years, and 0.51 (0.49 to 0.53) for ≥30 years. The incidence per 100 000 person years among the 0-14 years group was 1.72 (1.58 to 1.86) among males and 2.21 (2.05 to 2.39) among females (P<0.001, χ2=19.58). The incidence per 100 000 person years among the population aged ≥15 years was 0.92 (0.89 to 0.96) among males and 0.70 (0.67 to 0.74) among females (P<0.001, χ2=68.22).
Incidence of type 1 diabetes in different age groups in 13 areas of China
The estimated incidence of type 1 diabetes per 100 000 persons years for all ages varied from 0.52 (0.47 to 0.59) in Chengdu to 1.57 (1.38 to 1.79) in Lanzhou. For the 0-14 years group, the estimated incidence per 100 000 persons years varied from 1.14 in Chengdu (0.91 to 1.42) to 3.59 in Harbin (3.1 to 4.16). The incidence in the 0-14 years group was positively correlated with latitude (r=0.88, P<0.001). The estimated incidence per 100 000 person years for the 15-29 years group varied from 0.14 in Yinchuan (0.1 to 0.19) to 2.43 in Harbin (2.16 to 2.75) and for the ≥30 years group varied from 0.03 in Yinchuan (0.02 to 0.05) to 0.77 in Wuhan (0.67 to 0.89). The latitude related correlations were not observed in the last two age groups (15-29 years: r=0.49, P=0.09; ≥30 years: r=0.03, P=0.92) (see supplementary table S4).
Table 2 summarises the incidence of type 1 diabetes in the different age groups. Among the under 15s, the incidence peak was observed in the 10-14 years group (incidence per 100 000 person years 1.10 (0.97 to 1.24), 1.98 (1.80 to 2.18), 2.68 (2.47 to 2.91), for age groups 0-4 years, 5-9 years, and 10-14 years, respectively). For groups aged more than 15 years, the incidence of type 1 diabetes decreased steadily with age (P<0.001, χ2=989.54).
Based on previous reports1920212223 on factors affecting the incidence of type 1 diabetes and data availability, we performed correlation analysis and revealed that age group, latitude, and exposure to sunlight (as represented by average peak sunlight time (kWh/m2/day)) was statistically significantly correlated with incidence (see supplementary materials, section 6). Using a Poisson model including these three factors as covariates and population size as weight, the annual incidence of type 1 diabetes across China based on the 13 study areas was 1.01 (0.18 to 1.84) per 100 000 person years. The incidence rates for ages 0-14 years, 15-29 years, and ≥30 years were 1.93 (0.83 to 3.03), 1.28 (0.45 to 2.11), and 0.69 (0.00 to 1.51) per 100 000 person years, respectively.
Table 3 summarises the characteristics of type 1 diabetes at diagnosis in different age groups from medical record databases. Overall, 4661 new cases of type 1 diabetes were ascertained from medical record databases, including 1143 people aged 0-14 years, 1664 aged 15-29 years, and 1854 aged ≥30 years. Insulin treatment was started immediately in 98.4% of participants in the 0-14 years group, 93.5% in the 15-29 years group, and 91.5% in the ≥30 years group (P<0.001, χ2=59.76). The incidence rates of diabetic ketosis and diabetic ketoacidosis within six months of diagnosis were highest among the 0-14 years group (92.9%/51.4%), followed by the 15-29 years group (89.0%/43.0%), and lowest in the ≥30 years group (83.8%/30.8%) (diabetic ketosis: P<0.001, χ2=57.71; diabetic ketoacidosis: P<0.001, χ2=125.72). The proportions of cases with non-detectable fasting C peptide levels (<0.2 ng/mL) differed among the three age groups (22.5% v 21.7% v 27.5%, P=0.001, χ2=13.88). Data were collected on diabetes autoantibodies, including glutamate decarboxylase, the insulin antigen 2, islet cell antibody, insulin antibody, and the zinc transporter 8, tested under standardised procedures. The proportion of patients with at least one positive test result for diabetes autoantibodies showed a non-significant tendency to decrease with age (0-14 years (73.5%), 15-29 years (59.5%), ≥30 years (55.4%), P=0.22, χ2=3.16).
Clinical characteristics of participants with onset of type 1 diabetes
Discussion
China remains one of the countries with the lowest incidence of type 1 diabetes. In our study from 2010 to 2013 we found that although type 1 diabetes tends to develop in children, most of the new cases are diagnosed in adults. Furthermore, higher latitude is correlated with a higher incidence of type 1 diabetes in under 15s, but not in older population groups. We also noticed a high prevalence of diabetic ketoacidosis in participants ascertained within six months of diagnosis during our study period.
Low incidence of type 1 diabetes in China
Our study confirms that the incidence of type 1 diabetes remains low in China, even after the 3.8-fold increase of what was reported by the DiaMond Project two decades ago. Although the underlying mechanism is not completely known, the low incidence in China is probably attributed to genetic, environmental, and behavioural factors. A difference in prevalence of type 1 diabetes associated human leucocyte antigen genotypes has been reported to attribute to the difference in susceptibility to type 1 diabetes.24 However, other genes and environmental factors could also have an influence. Our study population has a homogenous gene background: a population of Han people. Intriguingly, when we compared the northern areas with the southern areas we observed up to a threefold difference in incidence of type 1 diabetes in the 0-14 years group. Finland is a country of high latitude (around 60.1°N), which may contribute to a higher incidence of type 1 diabetes. But if we compare the incidence in Finland25 with that in Harbin in northern China (45.8°N), it is still much lower (64.9 v 3.59 per 100 000 person years). This suggests that other factors, such as genetics, play a more important role in the incidence of type 1 diabetes.
Age and incidence
In our study the incidence of type 1 diabetes in under 15s during 2010 and 2013 was 1.93 (95% confidence interval 0.83 to 3.03) per 100 000 person years, presenting a 3.8-fold increase over that reported by the DiaMond study3 in the 1990s, equal to a roughly 6.5% annual increase. This increase appears to be rapid compared with those reported by the EURODIAB (3.3%)26 and SEARCH (1.8%) studies.5 However, we did not measure the trends in incidence. In fact we compared our results with the incidence reported in China in 1998.3 These results were from part of the DiaMond study, which may be underestimated as a result of incomplete ascertainment, as some of the participating centres reported small case numbers. Thus the apparent increase should be interpreted with caution. China remains one of the countries with the lowest incidence of type 1 diabetes globally, despite the increasing trend. None the less, considering its large population, China has the largest estimated number of new annual cases of type 1 diabetes in children, at 4271 of the estimated 10 000 in the West-Pacific region in 2015.27
In our study we found that most new cases of type 1 diabetes presented in adulthood. Indeed, approximately 65.3% of newly diagnosed cases were in participants aged more than 20 years. Our estimates for incidence of type 1 diabetes for all ages is 1.01 per 100 000 person years, and the incidence in the study areas for ages 20-29 years was 1.15 per 100 000 person years. Previous reported nationwide incidence rates at ages 20-29 years varies from 3.4 (Iran, 1990-94)28 to 19.4 (Kronoberg, Sweden, 1998-2001)29 globally. Although the paucity of type 1 diabetes incidence among all age groups makes comparison with other studies difficult, our estimates in both children and adults in China were among the lowest reported in the world. Nevertheless, we estimate that 9605 new cases occur annually in the population aged 15 or more years in China. This finding highlights the importance of the care of people with adult onset type 1 diabetes and that more resources should be provided to improve the care of this age group.
The age distribution of incidence of type 1 diabetes showed that the age of onset increases during childhood and then steadily decreases towards adulthood (table 2). The incidence rose to a peak of 2.68 per 100 000 person years in the 10-14 years group, consistent with rates reported by the DiaMond Project,1 the USA,5 and Japan30 in different periods. Most epidemiology studies that reported incidence in both childhood and adult type 1 diabetes observed the peak appearing close to puberty. However, studies from the USA31 and Europe32 described bimodal incidences, with the first peak in ages 10-14 years and the second peak around age 50 years. Such a peak around age 50 years was not observed in our study.
Sex and incidence
Our data show that the incidence of type 1 diabetes was higher among girls aged 0-14 years, consistent with previous reports. Two international type 1 diabetes registries (EURODIAB and DiaMond)24 showed that the overall sex ratio for incidence of type 1 diabetes is roughly equal in children, with a minor excess in males in regions with a high incidence (populations of European origin) and an excess in females in regions with a low incidence (populations of non-European origin) such as Asia and Africa. Several reports333435 indicate an excess in males among adults in populations of European origin. In contrast with the incidence of type 1 diabetes in children where an excess in girls was observed, we found that the incidence of type 1 diabetes in the population aged ≥15 years was greater in men than in women, consistent with previous findings. Different effects of environmental risk factors and lifestyle on incidence of type 1 diabetes in females and males were possible explanations for this difference.33 Such a difference may also suggest that childhood onset and adult onset type 1 diabetes have different manifestations in the sexes.
Latitude and incidence
Our results showed that the incidence of type 1 diabetes among children aged 0-14 years was strongly correlated with latitude, with higher rates in the north and lower in the south, but such correlation was not observed in participants aged ≥15 years. Previously reported effects of latitude on incidence of type 1 diabetes among young people are inconsistent. The EURODIAB study reported that the incidence of type 1 diabetes in childhood was positively correlated with latitude,36 whereas the SEARCH study did not show similar trends.37 The correlation between latitude and incidence in the younger but not the older population has not been reported previously. The difference between childhood onset and adult onset type 1 diabetes regarding the latitude effects on incidence may suggest different triggers for these two disease forms.
Although gene pools of the populations, ultraviolet radiation level in different regions, and the prevalence of virus infections have been postulated to be responsible for the correlation between latitude and incidence of type 1 diabetes among under 15s,19 the actual mechanism remains controversial. It has been reported that the Han population could be divided into three regional groups (northern, central, and southern) by variance in several loci of single nucleotide polymorphisms, including some in the human leucocyte antigen region previously reported to be related to psoriasis.38 Although the association between this variance and the development of type 1 diabetes is yet unknown, it is worthy of further study to clarify whether such variance is related to the incidence of type 1 diabetes.
Prevalence of diabetic ketoacidosis in cases of type 1 diabetes
Compared with other studies, ranging from no more than 15% (Sweden) to around 30% (the SEARCH study and the EURODIAB study) in young people with a diagnosis of diabetes,39 we observed a relatively high prevalence of diabetic ketoacidosis (40.1% in all age groups and 51.4% in under 15s) in participants with newly diagnosed type 1 diabetes during the study period. We collected the data on diabetic ketoacidosis occurring within six months of diagnosis. These episodes of diabetic ketoacidosis might occur at onset or after onset, reflecting different situations. Occurrence at onset of type 1 diabetes could be attributed to the acute onset of the disease or to the lack of awareness of the signs or symptoms of the disease by patients or healthcare providers. Diabetic ketoacidosis after onset but within six months of diagnosis could have been the result of insufficient education of the participant about diabetes or missing an injection of insulin. The high prevalence of diabetic ketoacidosis within six months of a diagnosis of type 1 diabetes in our study indicates that more effort and resources are needed to achieve earlier diagnosis, raise awareness, and improve education about type 1 diabetes in China.
Strengths and weaknesses of this study
We report the first population based registry study of incidence of type 1 diabetes in China in the past two decades. Our study is also the first nationwide study to provide incidence rates for type 1 diabetes in all age groups, covering a vast geographical area. These results should not only update the global map of type 1 diabetes in childhood, but also fill in the blank about the incidence of adult onset type 1 diabetes.
It has been a huge challenge to ascertain cases of type 1 diabetes. Although we were not able to utilise all the data from the medical insurance system owing to the inability to distinguish people with type 1 diabetes from those with type 2 diabetes, we had established a pharmacy based registry system and had utilised self report data from communities of patients with diabetes. Therefore, we believe that we have given as accurate an estimation as possible.
Several weaknesses of our study should be considered. The population we covered would provide enough power to estimate the incidence over 1.0 per 100 000 person years, but for the exceedingly low incidence rate of adult onset type 1 diabetes, especially in groups aged more than 40 years, a larger study population would be required to give a more accurate estimate. The study areas have a higher proportion of urban populations than that of the whole nation. This hindered us from studying the association between incidence of type 1 diabetes and environmental factors. However, correlation analysis showed no statistically significant association between incidence and the proportion of urban population (see supplementary table S4). Like most of the epidemiological studies in type 1 diabetes, the diagnosis in our study was a clinical one. We adopted a search strategy based on ICD (international classification of diseases, ninth and 10th revisions) codes and the diagnosis largely relied on our participating endocrinologists and paediatricians (see supplementary materials, section 3). This could result in missing cases or misdiagnosis. However, we took multiple steps to minimise such a possibility. We included all cases of diabetes in under 15s regardless of classification and diabetes coded as “unclassified” in all age participants when we searched with ICD codes to avoid any missing cases. Clinical information (presence of diabetes related symptoms, incidence of diabetic ketosis or diabetic ketoacidosis within six months of diagnosis, etc), and laboratory test results (including C peptide level and diabetic autoantibodies) were collected when available to assist the diagnosis. Finally, we ensured that the diagnostic time window for cases included in our study was no less than 18 months.
Conclusions
We found a rapid increase in the incidence of type 1 diabetes in under 15s in the past two decades in China, a country with a low incidence for this disease. We estimated that more than 13 000 new cases of type 1 diabetes occur every year in China, with more than 9000 in people aged 15 or more. Furthermore, we found that the incidence of type 1 diabetes was positively associated with higher latitude in under 15s, but not in the older population.
What is already known on this topic
The only available data on incidence of type 1 diabetes in China was provided by the DiaMond Project, reporting 0.51 and 0.59 per 100 000 person years among under 15s in 1985-94 and 1988-96, respectively
Most epidemiological studies worldwide have focused on onset of type 1 diabetes in childhood
A paucity of information thus exists on incidence of type 1 diabetes spanning all ages
What this study adds
The estimated incidence of type 1 diabetes per 100 000 persons years was 1.93 for 0-14 years, and 1.01 for all ages. Most new cases of type 1 diabetes in China are in adults
The incidence rates in under 15s were positively correlated with latitude
More resources should be provided to improve the care of people with onset of type 1 diabetes in adulthood
Author details
Acknowledgments
Jianping Weng, Zhiguang Zhou, Lixin Guo, Dalong Zhu, Linong Ji, Xiaoping Luo, Yiming Mu, Weiping Jia, Wenying Yang, Hongyu Kuang, Qiang Li, Yanbing Li, Li Yuan, Xuefeng Yu, Zhongyan Shan, Qiuhe Ji, Xingwu Ran, Jing Liu, Jiajun Zhao, Li Chen, Lanjie He, Chunxiu Gong, Li Liu, Feihong Luo, Ying Xin, Xueying Zheng, Daizhi Yang, Sihui Luo, Jinhua Yan, Elizabeth J Mayer-Davis
Jianping Weng,* Chang Jiang scholar, professor, head of Department of Endocrinology and Metabolism, Sun Yat-sen University Third Hospital, Guangdong Provincial Key Laboratory of Diabetology; Zhiguang Zhou,* professor, director of Endocrinology Department, the Second Xiangya Hospital, Central South University, Institute of Endocrinology and Metabolism; Lixin Guo,* professor, director of Endocrinology Department, Beijing Hospital; Dalong Zhu, professor, director of Internal Medicine and Endocrinology Department, Nanjing University Medical School Affiliated Nanjing Drum Tower Hospital; Linong Ji, professor, director of Endocrinology Department, Peking University People’s Hospital, Department of Endocrinology and Metabolism; Xiaoping Luo, professor, director of Pediatric Department, Tongji Hospital of Tongji Medical College, Huazhong University of Science & Technology; Yiming Mu, professor, director of Endocrinology Department, People’s Liberation Army General Hospital, China; Weiping Jia, professor, director of Endocrinology Department, The Sixth Affiliated People’s Hospital, Shanghai Jiao Tong University; Wenying Yang, professor, director of Endocrinology and Metabolic Diseases Centre, China Japan Friendship Hospital, Endocrinology; Hongyu Kuang, professor, director of Endocrinology Department, The First Affiliated Hospital of Harbin Medical University; Qiang Li, professor, director of Endocrinology Department, The Second Affiliated Hospital of Harbin Medical University; Yanbing Li, professor, director of Endocrinology Department, The First Affiliated Hospital of Sun Yat-sen University; Li Yuan, professor, director of Endocrinology Research, Union Hospital, Tongji Medical College, Huazhong University of Science & Technology; Xuefeng Yu, professor, director of Endocrinology Department, Wuhan Tongji Hospital, China; Zhongyan Shan, professor, director of Endocrinology Department, First Affiliated Hospital, Chinese Medical University; Qiuhe Ji, professor, director of Endocrinology Department, Xijing Hospital, Fourth Military Medical University; Xingwu Ran, professor, deputy director of Endocrinology Department, West China Hospital of Sichuan University, Diabetic Foot Care Center, Department of Endocrinology and Metabolism; Jing Liu, professor, director of Endocrinology Department, Gansu Provincial Hospital; Jiajun Zhao, professor, director of Endocrinology Department, Shandong Provincial Hospital; Li Chen, professor, director of Endocrinology Department, Qilu Hospital of Shandong University; Lanjie He, professor, director of Special Care Department, General Hospital of Ningxia Medical University; Chunxiu Gong, professor, director of Centre of Endocrinology, Genetics and Metabolism, Beijing Children’s Hospital, Capital Medical University, Endocrinology, genetics and metabolism; Li Liu, professor, director of Department of Endocrinology and Metabolism, Guangzhou Women and Children’s Medical Center; Feihong Luo, professor, director of Department of Endocrinology, Genetics and Metabolism, Children’s Hospital of Shanghai; Ying Xin, professor, director of Department of Children’s Endocrinology and Metabolism, Shengjing Hospital of China Medical University; Xueying Zheng, physician, Third Affiliated Hospital of Sun Yat-Sen University, Guangdong Provincial Key Laboratory of Diabetology; Daizhi Yang, physician, the Third Affiliated Hospital of Sun Yat-Sen University, Department of Endocrinology and Metabolic Disease, Guangdong Provincial Key Laboratory of Diabetology; Sihui Luo, physician, the Third Affiliated Hospital of Sun Yat-Sen University, Department of Endocrinology and Metabolic Disease; Jinhua Yan, associate chief physician, the Third Affiliated Hospital of Sun Yat-Sen University, Department of Endocrinology and Metabolic Disease, Guangdong Provincial Key Laboratory of Diabetology; Elizabeth Mayer-Davis, Cary C Boshamer distinguished professor of nutrition and medicine, chair of Department of Nutrition, University of North Carolina at Chapel Hill. *These authors contributed equally to the study.
The T1D China study is officially authorised by the Bureau of Medical Administration, Inspection and Supervision of National Health and Family Planning Commission of the People’s Republic of China, funded by China International Medical Foundation and supervised by the Chinese Medical Association. We thank our healthcare providers from the 505 hospitals and patients and their families from diabetes communities for participating in this study; we thank for their advice the consultant committee members including Jialun Chen and Manyin Xu from Ruijin Hospital Shanghai Jiao Tong University; Kunsan Xiang from Shanghai Jiao Tong University Affiliated Sixth People’s Hospital; Changyu Pan from Chinese PLA General Hospital; Xiujun Li from West China Hospital Sichuan University; Jiawei Chen from Jiangsu Province Hospital; and Guang Ning from the Chinese Society of Endocrinology; and we thank Xueqin Wang from Sun Yat-sen University and Jasmin Divers from Wake Forest University, USA for their statistical assistance.
Footnotes
Contributors: JW, ZZ, and LG are joint first authors. JW designed and organised the study and cowrote the first draft of the manuscript. JY assisted JW to run the study, collect data in the study site, interpret the data, and cowrite the first draft. ZZ and LG assisted in the design and organisation of the study, and contributed in manuscript discussion. DZ, LJ, XL, YM, WJ, WY, HK, QL, YL, LY, XY, ZS, QJ, XR, JL, JZ, LC, LH, CG, LL, FL, and YX organised the study in their study regions and contributed to the data collection. LJ, DZ, ZS, and XL also contributed in data interpretation. HK, XJ, XR, and JL also contributed to data analysis. XZ, DY, and SL contributed to the data analysis, data interpretation, and manuscript discussion. EM advised on study design and contributed to the manuscript discussion. The corresponding author (JW) had full access to all the data in the study and had final responsibility for the decision on content and publication submission. All authors have seen and approved the final text. The funder of the study had no role in the study design; data collection, analysis, or interpretation; or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication. JW, ZZ, and LG are the guarantors.
Funding: This study was funded by the China International Medical Foundation, national key R&D programme of China (2017YFC1309603, 1309602), and National Natural Science Foundation of China (key programme 81530025).
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author). No financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: The protocol was reviewed and approved by the institutional review boards of the Third Affiliated Hospital of Sun Yat-sen University.
Data sharing: No additional data available.
Transparency: The lead author (JPW) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.