Article Text

Abstract
Background The association of long-term effects of inorganic arsenic (iAs) exposure with type 2 diabetes mellitus (T2DM) risk remains controversial.
Methods A literature search was performed in PubMed, China National Knowledge Infrastructure and Web of Knowledge for relevant available articles published in English or Chinese from 1 January 1990 to 5 June 2013. Case-control, cohort or cross-sectional studies evaluating iAs and T2DM were included. The DerSimonian and Laird random effect model was adopted as the pooling method. Dose-response relationship was assessed by restricted cubic spline model and multivariate random-effect meta-regression.
Results Of the 569 articles identified through searching databases, 17 published articles with 2 243 745 participants for iAs in drinking water and 21 083 participants for total arsenic (tAs) in urine were included for this meta-analysis. The pooled relative risk with 95% CI of T2DM for the highest versus lowest category of iAs exposure level in drinking water was 1.75 (1.20 to 2.54). After removing three studies that had a strong effect on heterogeneity, the pooled relative risk was 1.23 (1.12 to 1.36). Dose–response analysis suggested T2DM risk increased by 13% (1.13 (1.00 to 1.27)) for every 100 µg/L increment of iAs in drinking water. Significant association of T2DM risk with tAs in urine was also found 1.28 (1.14 to 1.44).
Conclusions This meta-analysis indicates that long-term iAs exposure might be positively associated with T2DM risk.
- TOXICOLOGY
- SYSTEMATIC REVIEWS
- Environmental epidemiology
- PUBLIC HEALTH
- EPIDEMIOLOGY
Statistics from Altmetric.com
Introduction
According to the reports of the WHO in 2011, diabetes affects an estimated 346 million people globally. Type 2 diabetes mellitus (T2DM) accounts for 90%–95% of all cases of diabetes, and is predicted to affect a total of 366 million people by 2030.1 Several risk factors might be associated with T2DM, such as older age, sex, obesity, physical inactivity, family history and psychosocial stress.2–4 In addition, toxic elements, such as inorganic arsenic (iAs), occurring in ground water worldwide,5 have been recently proposed as risk factors for T2DM.6
Several studies based on populations have been performed to assess the association of iAs exposure with T2DM risk. According to several studies conducted in endemic arsenic exposure areas such as Taiwan and Serbia, iAs in drinking water was associated with an increased T2DM risk.7–9 However, other studies conducted in China and Cyprus found no association between them.10 ,11 And the relationship between total arsenic (tAs) in urine and T2DM risk remains controversial.12–18 Overall, the epidemiological evidence is insufficient and inadequate to establish whether the association between iAs exposure and T2DM risk exists.
Therefore, we performed a meta-analysis to: (1) assess the effect of iAs exposure on T2DM risk, including iAs in drinking water and urine; (2) evaluate the possible dose–response relationship of iAs in drinking water with T2DM risk; (3) explore the potential between-study heterogeneity; and (4) explore the potential small-study effect.
Materials and methods
We referred to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting of meta-analyses in this analysis.
Search strategy
A literature search from 1 January 1990 to 5 June 2013 was conducted by two investigators (WJW, DFZ) independently for relevant available articles published in English or Chinese from three databases: (1) PubMed; (2) China National Knowledge Infrastructure (CNKI); (3) Web of Knowledge. The search terms included ‘environmental exposure’, ‘arsenic’, ‘inorganic arsenic’, ‘diabetes’, ‘DM’ and ‘T2DM’. Moreover, we also reviewed the references of the included studies to identify additional studies not captured by our database searches. The flow diagram of literature search was shown in figure 1, and see the full search text in online supplementary appendix.

Flow diagram of literature search.
Inclusion criteria
The inclusion criteria were as follows: (1) case-control, cohort or cross-sectional studies published as the original study; (2) the exposure of interest was iAs; (3) the outcome of interest was T2DM; (4) relative risk (RR) with corresponding 95% CI (or data to calculate these) were reported; (5) the most recent and complete article was chosen if a study had been published more than once. T2DM cases were defined as self-reported physician diagnosis, taking insulin or oral hypoglycaemic drugs, fasting glucose test or 75-g oral glucose tolerance test.
All identified studies were carefully reviewed independently by two investigators to identify and determine whether an individual study was eligible for inclusion criteria in this meta-analysis. If the two reviewers could not reach a consensus about the eligibility of an article, it was resolved by disputing with a third investigator.
Data extraction
Data were independently extracted by two investigators (WJW, ZTX) who reached a consensus on all of the items, with disagreements resolved through discussion. And the data were reviewed by a third investigator (YL). Information extracted from each study was as follows: publication year, the first author’s name, country where the study was performed, study design, sample size and number of cases, mean age, male percentage in case (exposed) and control (unexposed) groups, definition of cases, cut-points for arsenic exposure, RRs (we presented all results with RR for simplicity) with corresponding 95% CIs for the highest versus lowest categories of iAs exposure and variables adjusted for in the analysis. The RRs adjusted with the most confounders in the original studies were extracted.
Statistical analysis
Pooled measure was calculated to assess the strength of association between iAs exposure and T2DM risk. The studies on iAs in drinking water and tAs in urine would be assessed separately. The I2 19 was used to assess heterogeneity among studies. The random effect model (REM) was adopted as the pooling method. Meta-regression was performed to assess the potentially important covariates that might exert substantial impacts on between-study heterogeneity. The ‘leave one-out’ sensitive analysis20 was carried out to evaluate the key studies that have substantial impact on the between-study heterogeneity. An analysis of influence was conducted,21 which describes how robust the pooled estimator is to removal of individual studies. Small study effect was assessed with visual inspection of the funnel plot and Begg test.22
For dose–response analysis, a two-stage random-effects dose–response meta-analysis23 was performed. In the first stage, a restricted cubic spline model with three knots at the 25th, 50th, and 75th centiles24 of the levels of iAs in drinking water was estimated using generalised least square regression, taking into account the correlation within each set of published RRs.25 Then the study-specific estimates were combined using the restricted maximum likelihood method in a multivariate random-effects meta-analysis.26 A p value for nonlinearity was calculated by testing the null hypothesis that the coefficient of the second spline is equal to 0. All statistical analyses were performed with STATA V.10.0 (Stata Corporation, College Station, Texas, USA). All reported probabilities (p values) were two-sided, with p≤0.05 considered statistically significant.
Results
Characteristics of studies
We identified 17 published articles7–18 27–31 eligible for this meta-analysis on the relationship of iAs exposure with T2DM risk, including 12 studies with 2 243 745 participants for iAs in drinking water and 7 studies with 21 083 participants for tAs in urine. The number of study designs for case-control, cohort and cross-sectional studies was 3, 3 and 11, respectively. The baseline characteristics of the study participants and design characteristics in the published articles are shown in tables 1 and 2.
Characteristics of studies for iAs in drinking water included in the meta-analysis
Characteristics of studies for tAs in urine included in the meta-analysis
Quantitative synthesis
The results of the pooled analysis for iAs in drinking water are summarised in figure 2. Among the 12 studies on iAs in drinking water, all the studies reported a positive association (ie, RR >1.00), with 7 of them being statistically significant. The pooled RR was 1.75 (95% CI 1.20 to 2.54; I2 = 95.90%; REM; pheterogeneity< 0.05).
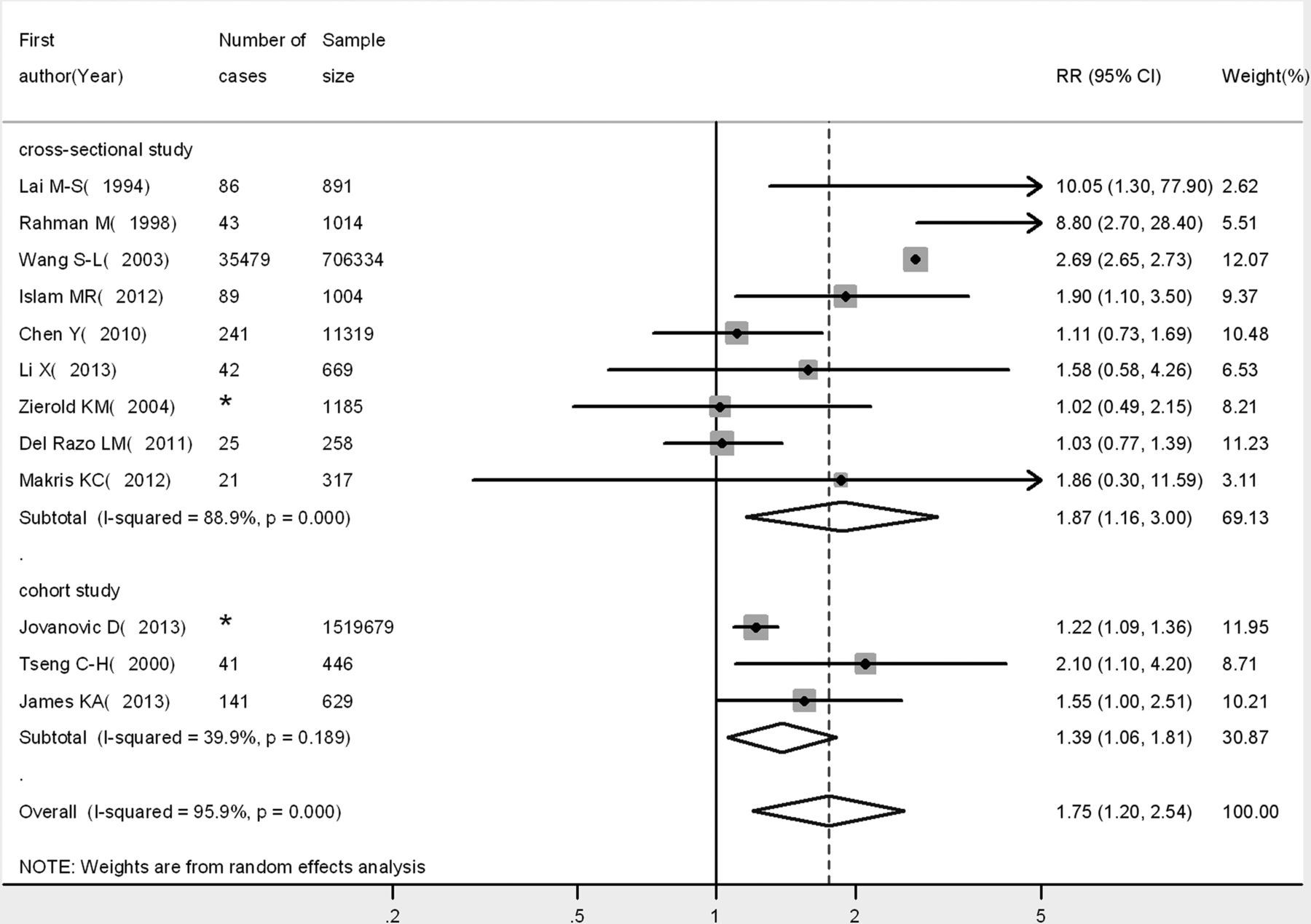
Forest plot of the relative risks (RRs) with corresponding 95% CIs of studies on iAs in drinking water and type 2 diabetes mellitus. The size of grey box is positively proportional to the weight assigned to each study, which is inversely proportional to the SE of the RR, and horizontal lines represent the 95% CIs. *, not available. Access the article online to view this figure in colour.
We conducted a subgroup analysis stratified by study design for iAs in drinking water. The pooled RRs for cohort and cross-sectional studies were 1.39 (95% CI 1.06 to 1.81; I2 = 39.90%;REM; pheterogeneity=0.19) and 1.87 (95% CI 1.16 to 3.00; I2 = 88.90%;REM; pheterogeneity < 0.05), respectively (figure 2).
For dose–response analysis, data from four studies 11 ,14 ,27 ,30 were used including 410 T2DM cases. A linear relationship was found of iAs in drinking water with T2DM risk (p for nonlinearity=0.47), and the RRs (95% CI) of T2DM were 1.00 (0.95 to 1.06), 1.10 (0.82 to 1.48), 1.31 (1.01 to 1.70), 1.63 (1.24 to 2.15) and 3.13 (1.68 to 5.85) for 16, 147, 250, 376 and 750 µg/L compared with 0 µg/L. In addition, the dose–response analysis suggested that T2DM risk increased by 13% (1.13 (1.00 to 1.27)) for every 100 µg/L increment for iAs in drinking water (figure 3).

The dose–response analysis between iAs in drinking water and type 2 diabetes mellitus risk with restricted cubic splines in a multivariate random-effects dose–response model. The solid line and the long dash line represent the estimated relative risks and its 95% CIs. Short dash line represents the linear relationship.
Among the seven studies on tAs in urine, six studies reported a positive association, with three of them being statistically significant. Only one study reported a negative association (ie, RR < 1.00), but this value was not statistically significant. Overall, significant association was also found between tAs in urine and T2DM risk with the pooled RR of 1.28 (95% CI 1.14 to 1.44; I2 = 6.70%; REM; pheterogeneity=0.38) (figure 4).

Forest plot of the relative risks (RRs) with corresponding 95% CIs of studies on tAs in urine and type 2 diabetes mellitus. The size of grey box is positively proportional to the weight assigned to each study, which is inversely proportional to the SE of the RR, and horizontal lines represent the 95% CIs. Access the article online to view this figure in colour.
We also conducted a subgroup analysis stratified by study design for tAs in urine. The pooled RRs for case-control and cross-sectional studies were 1.51 (95% CI 1.00 to 2.26; I2=58.30%; REM; pheterogeneity=0.09) and 1.26 (95% CI 1.13 to 1.40; I2 = 0.0%; REM; pheterogeneity=0.79) (figure 4).
Sources of heterogeneity and sensitive analysis
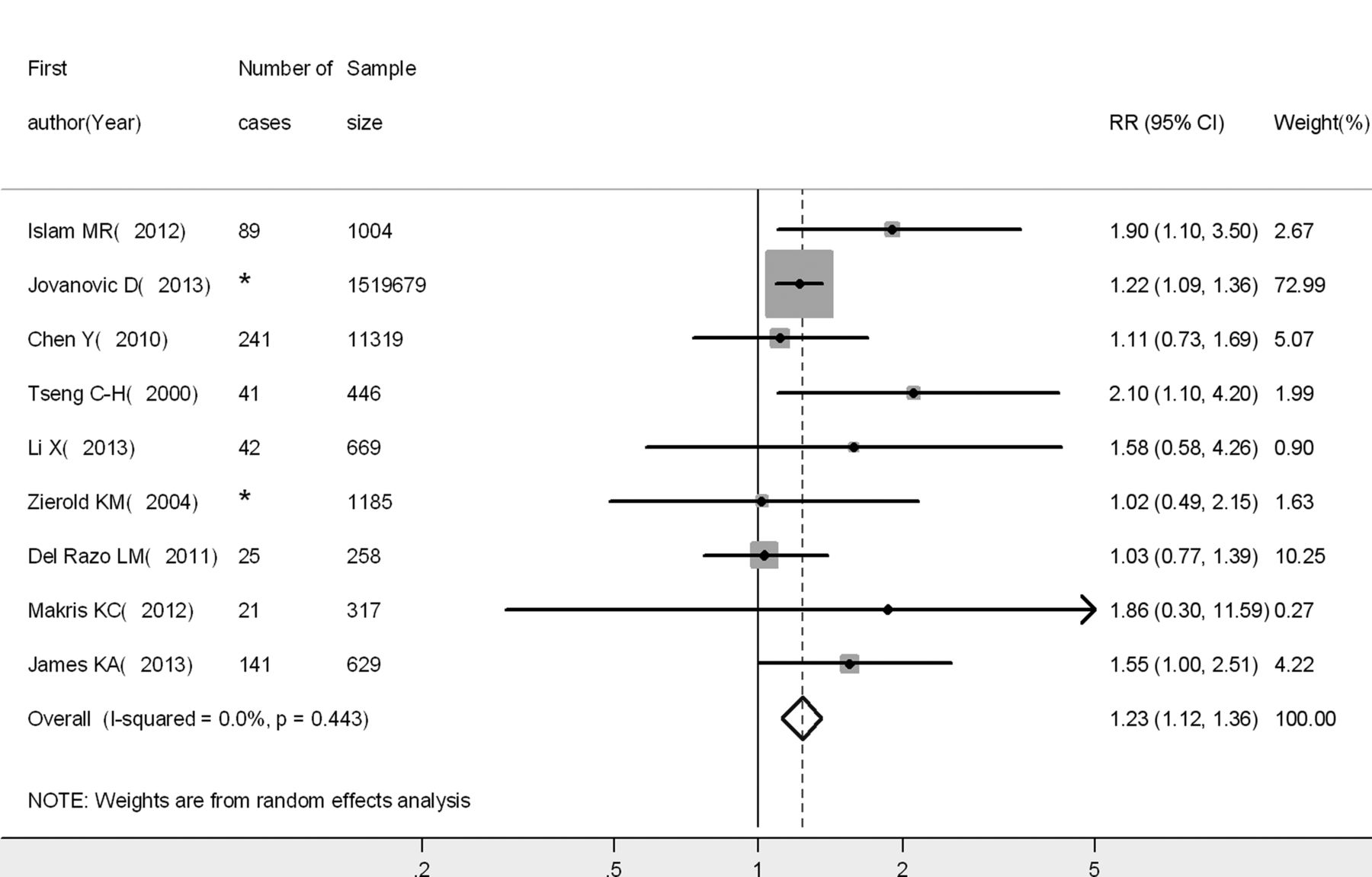
As seen in figure 2, strong evidence of heterogeneity among studies was demonstrated for iAs in drinking water with T2DM. However, univariate meta-regression analysis, with the covariates of sex, age, study design, sample size or measurements of water iAs exposure showed no covariates having a significant impact on between-study heterogeneity (see online supplementary table S1). After excluding two articles (RR > 3.00) conducted by Lai et al7 and Rahman et al,27 the key article contributed to this high between-study heterogeneity assessed by the ‘leave one-out’ sensitive analysis was the one conducted by Wang et al.8 After further excluding this article, no heterogeneity (I2=0.0%) was found, and the pooled RR was 1.23 (95% CI 1.12 to 1.36; I2 = 0.00%; REM; p heterogeneity=0.44) (figure 5).
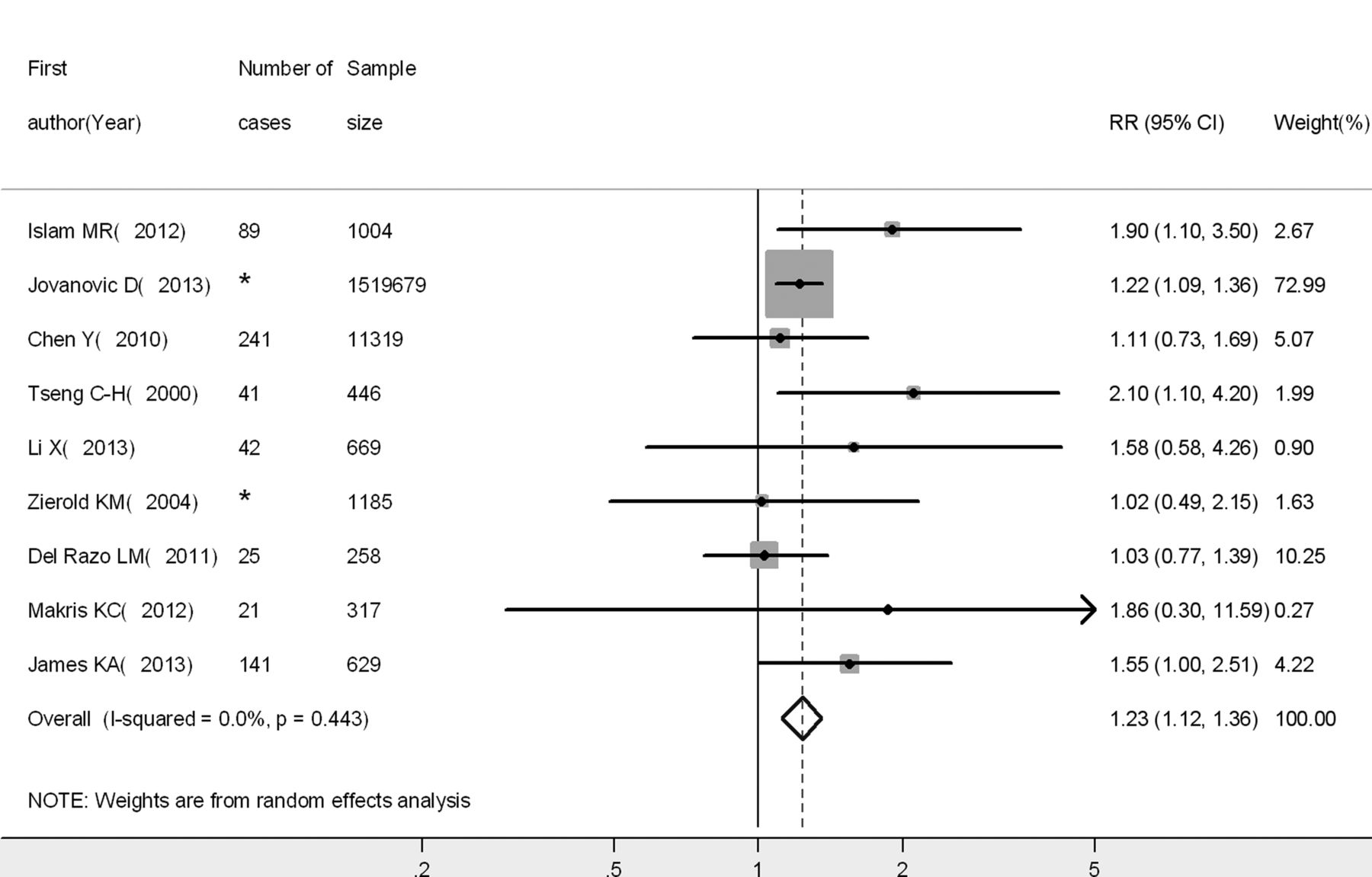
Forest plot of the relative risks (RRs) with corresponding 95% CIs of studies on iAs in drinking water and type 2 diabetes mellitus after sensitive analysis. The size of grey box is positively proportional to the weight assigned to each study, which is inversely proportional to the SE of the RR, and horizontal lines represent the 95% CIs. *, not available. Access the article online to view this figure in colour.
Influence analysis
No individual study was found to have excessive influence on the pooled effects for iAs in drinking water after sensitive analysis and for tAs in urine.
Small-study effect evaluation
The visual inspection of the funnel plot and Begg test showed that no evidence of significant small-study effect was found for tAs in urine (p=0.76). For iAs in drinking water, significant asymmetry of the funnel plot (small-study effect) was found in the Begg test (p=0.03) (figure 6); however, no significant small-study effect was found (p=0.47) after removing three studies that had a strong effect on heterogeneity (figure 7).
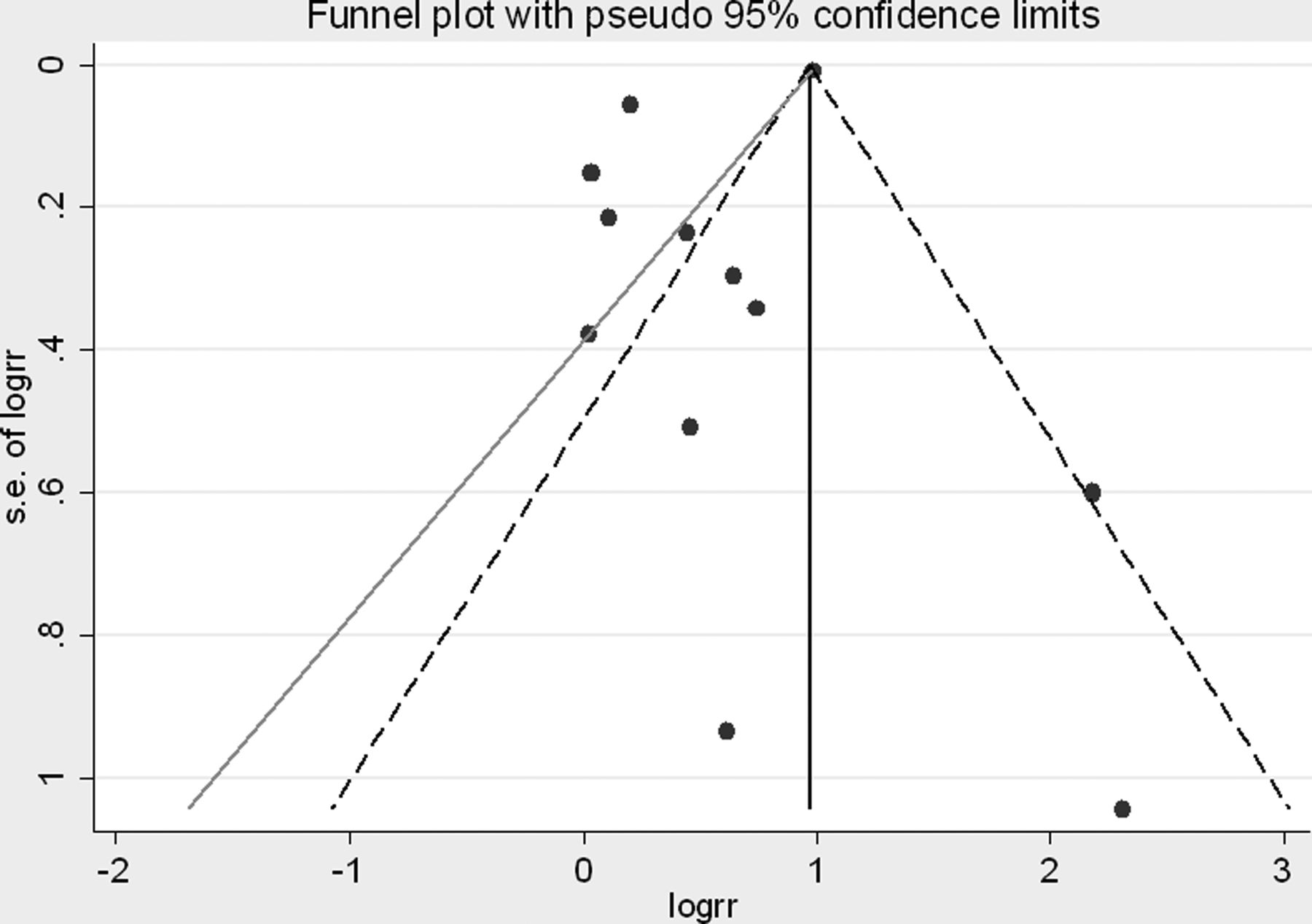
Funnel plot of the relative risks of 12 studies on iAs in drinking water and type 2 diabetes mellitus. Each dot represents a different study. Access the article online to view this figure in colour.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot of the relative risks of nine studies after removing three studies that had a strong effect on heterogeneity on iAs in drinking water and type 2 diabetes mellitus. Each dot represents a different study. Access the article online to view this figure in colour.
Proteus phenomenon
There was no Proteus phenomenon in our meta-analysis. No significant difference was identified between the RR of the first published study7 and the pooled RR of subsequent studies (p=0.08).The pooled RR of all studies decreased with time passing (β=−0.05), and the pooled RR of excluding first study showed the same tendency (β=−0.05).
Discussion
In recent years, many studies had been performed to evaluate the relationship between iAs exposure and T2DM risk based on populations. However, the results in the publications were conflicting. In general, individual study has a relatively small number of participants with underpower for detecting the effect; thus, meta-analysis should be the appropriate approach to obtain a more definitive conclusion. Our meta-analysis, including 2 243 745 participants for iAs in drinking water and 21 083 participants for tAs in urine, strongly identified the association of iAs exposure with increased T2DM risk. And dose–response analysis suggested T2DM risk increased by 13% (1.13 (1.00 to 1.27)) for every 100 µg/L increment of iAs in drinking water.
Between-study heterogeneity is common in meta-analysis,32 and it is essential to explore the potential sources of between-study heterogeneity. An indeterminate number of characteristics that varied among the studies could be the sources, such as age, sex, sample size, study design, design quality, different ranges of iAs exposure levels, different assessments of iAs exposure and other variation of the covariates in studies. Thus we used both meta-regression and the ‘leave one-out’ sensitive analysis that aimed to explore the potential important causes of the between-study heterogeneity. Our meta-analysis did not find the covariates of sex, age, sample size, study design or measurements of iAs exposure (for iAs in drinking water) as the important contributors to the between-study heterogeneity. After excluding two articles (RR > 3.00) conducted by Lai et al7 and Rahman et al,27 the key contributor of the article to this high between-study heterogeneity assessed by the ‘leave one-out’ sensitive analysis was the one conducted by Wang et al.8 As seen in figure 5, when we excluded these three articles, no heterogeneity (I2=0.0%) was found. After subgroup analysis and sensitive analysis, the results showed consistent positive association with the one based on all studies, strongly identifying the relationship of iAs exposure and T2DM risk. In this meta-analysis, no significant small-study effect was found. And what's more, there was no the Proteus phenomenon, which resulted in the appearance of extreme, contradictory findings very early during the accumulation of studies.
As a meta-analysis of relevant published studies, our study has several strengths. First, the quantitative assessments were based on a large sample size with 2 253 251 participants, thus reducing sampling error to a great extent. Second, the literatures search and data extraction was conducted independently by two investigators; therefore, the random error introduced by inserting data into tables was avoided greatly. Third, for iAs in drinking water, the pooled RR for cohort study was 1.39 (95% CI 1.06 to 1.81), strongly identifying the effect of iAs exposure on T2DM risk. Fourth, nearly all studies on iAs exposure levels had adjusted for major risk factors, including older age, obesity, physical inactivity and body mass index, indicating that the results were more credible. Fifth, after removing three studies that had a strong effect on heterogeneity, no evidence of significant small-study effect was found based on visual inspection of the funnel plot and Begg test for this meta-analysis. Sixth, after conducting the subgroup analysis and sensitive analysis, the results showed consistent positive association with the one based on all studies, strongly identifying the association stable.
Nevertheless, our study also has three limitations. First, because unknown confounders could not be excluded as potential explanations for the observed findings, inadequate control for confounders might bias the results in either direction, toward exaggeration or underestimation of risk estimates. Second, our results were likely to be affected by some misclassification of T2DM. Because the validity of glucometer has been a concern,33 ,34 inaccurate results might result from the use of a glucometer when measuring fasting plasma glucose levels in several studies.11 ,15 ,30 Third, although significant increased risk of T2DM associated with iAs >250 µg/L was found in the dose–response analysis, the observed threshold effect might arise from an effect of limited power, and no threshold effect would be found if infinite sample size was included. Thus, further studies with large sample size are still needed to further clarify the dose–response relationship.
To better understand the pathophysiology and mechanism of the diabetogenic effect of iAs, studies on biomarkers, such as HbA1c, are also needed. In addition, we should conduct more studies based on populations to identify the association between iAs exposure and T2DM risk, with more exact measurement of As species and levels.
In conclusion, this meta-analysis provides strong evidence that iAs exposure is a significant risk factor for T2DM. Given the high prevalence and incidence of T2DM in the general population, the observed association between iAs exposure and T2DM has clinical and public health importance.
What is already known on this subject
-
Inorganic arsenic, occurring in ground water worldwide, has been recently proposed as risk factor for T2DM.
-
Many studies have been performed to assess the association of inorganic arsenic exposure with T2DM risk.
-
However, the association remains controversial at present.
What this study adds
-
No meta-analysis of this association has yet been conducted.
-
This meta-analysis indicated that long-term inorganic arsenic exposure might be positively associated with T2DM risk.
-
Dose–response analysis suggested T2DM risk increased by 13% (1.13 (1.00 to 1.27)) for every 100 µg/L increment for inorganic arsenic in drinking water.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online table
Footnotes
-
Contributors WW and DZ conceived the study, participated in its design and coordination, carried out the literature searching and data extraction and were involved in drafting the manuscript or revising it critically for important intellectual content. ZX and YL carried out the literature searching, data extraction and interpretation of the data and were involved in drafting the manuscript. DZ was involved in interpretation of the data and revising the manuscript critically for important intellectual content.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.