Article Text

Abstract
Mouse models are frequently used to study diabetes-associated ulcers, however, whether these models accurately simulate impaired wound healing has not been thoroughly investigated. This systematic review aimed to determine whether wound healing is impaired in mouse models of diabetes and assess the quality of the past research. A systematic literature search was performed of publicly available databases to identify original articles examining wound healing in mouse models of diabetes. A meta-analysis was performed to examine the effect of diabetes on wound healing rate using random effect models. A meta-regression was performed to examine the effect of diabetes duration on wound healing impairment. The quality of the included studies was also assessed using two newly developed tools. 77 studies using eight different models of diabetes within 678 non-diabetic and 720 diabetic mice were included. Meta-analysis showed that wound healing was impaired in all eight models. Meta-regression suggested that longer duration of diabetes prior to wound induction was correlated with greater degree of wound healing impairment. Pairwise comparisons suggested that non-obese diabetic mice exhibited more severe wound healing impairment compared with db/db mice, streptozotocin-induced diabetic mice or high-fat fed mice at an intermediate stage of wound healing (p<0.01). Quality assessment suggested that the prior research frequently lacked incorporation of key clinically relevant characteristics. This systematic review suggested that impaired wound healing can be simulated in many different mouse models of diabetes but these require further refinement to become more clinically relevant.
- transgenic and knockout mice
- meta-analysis
- ulcer(s)
- laboratory research in diabetes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Diabetes-related foot disease (DFD) is a leading cause of impaired health-related quality of life, amputation, hospitalization and healthcare costs.1–6 The most common presentation of DFD is a foot ulcer which is estimated to develop in 10–20 million people worldwide annually.1 The lifetime incidence of foot ulceration in people with diabetes has been estimated as up to 30%.1 4 The mortality of patients with diabetes-related foot ulcers has been estimated to be 50% over 5 years and more than double that of people with diabetes but no foot ulcer.1 7 8 The development of improved understanding of diabetes-related ulcer pathogenesis and the discovery of novel treatments are therefore global priorities.
Animal models of human disease are commonly used to identify new treatments. There are many methods of inducing diabetes that have been used to study atherosclerosis, nephropathy and neuropathy in mice.9–11 There has, however, been limited focus on modeling DFD in mice. There is no current consensus on the most appropriate mouse model of diabetes-associated ulceration. A key requirement of a model of diabetes-associated ulceration is impaired wound healing. This has been attributed to several pathological processes stimulated by chronic hyperglycemia, including atherosclerosis and microvascular disease that lead to leg ischemia and peripheral neuropathy.12 13 It is not currently clear which of the different methods of inducing diabetes in mice are associated with wound healing impairment. In order to inform the appropriate choice of animal model, this review aimed to systematically examine the healing rates of wounds in mouse models of diabetes. The review also examined the quality and clinical relevance of this past research.
Methods
Search strategy, inclusion and exclusion criteria
This review was performed according to the 2015 Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols statement (online supplementary table 1).14 The protocol was registered in the PROSPERO database (Registration Number: CRD42018116224). Searches of the literature were conducted between 16 August 2018 and 24 January 2019 by one author (PH) on three separate occasions. The databases Medline, PubMed, Scopus, ScienceDirect and Web of Science were searched to identify preclinical studies examining the effects of diabetes on wound healing in mice. The full search strategy consisted of the terms (‘diabetic wound’ OR ‘diabetic foot ulcer’) AND (mouse OR mice OR murine) AND (nondiabetic OR non-diabetic OR normoglycemi* OR normoglycaemi*) using both Medical Subject Headings and keyword searches. The resultant articles were filtered in two stages, automatically using the database filters and manually by one author (PH) to only include original journal articles written in English. For inclusion, studies had to examine wound healing in mouse models of diabetes compared with age-matched controls and report wound area as a ratio or percentage of the initial wound area monitored over time for both groups.
Supplemental material
Data extraction and quality assessment of included studies
Full-text publications of included studies were independently assessed by two investigators (PH and JP). Data extracted included sex, age and strain of mice, model of diabetes, diagnostic criteria for diabetes, whether diabetes was confirmed prior to wound generation, the size and location of the initial wound, method and period of monitoring, and wound closure percentage defined as detailed below. ImageJ V.1.48 (National Institutes of Health, USA) was used to extrapolate data from figures if required. Extracted data were discussed in a consensus meeting.
The quality of the included studies was assessed using two tools specifically developed for this systematic review (online supplementary tables 2 and 3). One tool assessed the study design and reporting quality of the studies and was based on a prior tool,15 and the Animal Research: Reporting of In Vivo Experiments guidelines (online supplementary table 2). The second tool assessed the design of the mouse model experiment in relation to recognized characteristic features of human diabetes-associated ulcers (online supplementary table 3). Each checklist item was weighted equally and graded 0, 0.5 or 1 for no, unclear or yes, respectively. Each study was scored as a percentage of the total possible score for each tool.
Data analysis
The primary outcome of this systematic review and meta-analysis was percentage (%) wound closure which was calculated from extracted data using the following formula:
% Wound Closure
To gauge the effect of diabetes on wound closure over time, extracted data were sorted for analysis to early (2–5 days), intermediate (6–10 days) and late stages (11–20 days) of wound healing. In the event that a single article contained multiple independent animal studies, wound closure data were extracted from each of these studies and treated as independent data. If an article appeared to have multiple animal studies using the same mice in their experimental groups, sample sizes were evenly divided among them for meta-analysis to minimize duplication of data. For example, if primary outcome data were available for two different sets of diabetic mice but the authors used the same mice as controls for both, the sample size of the control group was evenly divided between the two diabetic groups for analysis. Corresponding authors of studies were contacted for key missing data. When necessary, SEMs were converted to SDs using GraphPad Prism V.7 (San Diego, California, USA). Meta-analyses were performed to assess the effect of diabetes on wound closure using Review Manager V.5.3.5 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014), while meta-regression analyses were performed using Open Meta-Analyst.16 Since heterogeneity between studies was expected, random effects models were used. Data were reported as standardized mean difference (SMD) with 95% CIs. Subgroup analyses were performed to examine whether the extent of wound healing impairment was different between the models of diabetes included. These pairwise comparisons were corrected for multiple testing using Bonferroni’s correction. Leave-one-out sensitivity analyses were also performed. The I2 index was used to assess the degree of heterogeneity between studies, with I2>50% accepted to denote statistical heterogeneity. Funnel plots of the effect size versus the SEM of the log-transformed effect were constructed to assess potential publication bias. A p value <0.05 was considered to be statistically significant.
Results
Study selection
After a systematic search, a total of 77 studies were included in this systematic review and meta-analysis (online supplementary figure 1).17–93
Characteristics of the included studies
The characteristics of the 77 included studies are shown in online supplementary table 4. There were a total of eight different mouse models of diabetes used (with three studies using multiple models).62 68 89 These included streptozotocin (STZ) injection (n=41; 20 single dose; 21 multiple doses), leptin receptor defective db/db mice (n=27), alloxan injection (n=4; 3 single dose; 1 multiple doses), high-fat fed mice (n=4), leptin-deficient ob/ob mice (n=2) and non-obese diabetic (NOD) mice (n=2). The majority of studies reported including male mice only (49/77). Eleven investigations included female mice only, two included mice of both sexes and the remaining studies did not report the sex of the mice included (15/77).
Only three studies examined wounds created in the hindlimb.37 51 61 The other studies investigated wounds created on the torso of mice (74 in total; 71 on the back, 3 on the flank). The initial wound size differed greatly between studies (online supplementary table 4). Ten studies used splints to prevent the closure of wounds via contraction and promote wound healing through re-epithelialization since this has been suggested to be more typical of humans.94 95
Quality of design and reporting of the included studies
The mean study design quality assessment score was 55.1% (range 19.2%–80.8%) (online supplementary table 5). Most studies (n=73) provided an ethics statement.23 Only nine studies reported that examination of wound closure was performed by an assessor blinded to group allocation. Only two studies indicated that investigators were blinded to the experimental groups of mice.17 72 Only three studies reported that power calculations were performed to determine appropriate sample sizes,32 37 47 while an additional two justified their sample sizes based on previous experiments.63 72
Forty-one studies did not report full information about the strain of mice used. Twelve studies did not indicate the start date of their studies,20 40–44 48 54 55 57 80 84 with an additional 27 only reporting the age of mice as ranges.17–19 21 23 24 26 28 29 36 39 49–53 60 62 73 78 79 81 87–90 93 Eighteen studies which investigated STZ-induced diabetes did not indicate whether non-diabetic mice were injected with vehicle.25 27 30 38 51 54 55 58 60–62 68 71 73 74 78 79 83 In studies which used genetic models of diabetes, 14 used homozygote mice of the background strain or non-diabetic littermates, as controls mice,19–21 23 24 29 45 46 50 52 70 81 82 89 while two studies did not indicate the use of littermate controls.40 56 Two studies described the wound closure measurements in the methods but represented their data in another way.70 85
Relevance of the reported mouse models to human diabetes-associated ulceration
The mean clinical relevance quality assessment score was 44.9% (range 26.9%–65.4%) (online supplementary table 6). Most studies (n=46) reported a clear diagnostic criterion for diabetes. This was mainly based on blood glucose concentrations. One study reported the confirmation of diabetes by the presence of glycosuria.20 Despite the Diabetic Complications Consortium recommendations for the appropriate confirmation of diabetes in animal models, only 15 of the 46 studies reported blood glucose measurements were performed in fasted mice18 25 33 35 38 65–69 72 76 77 81 91 and only three reported monitoring additional diabetes-associated metabolic parameters, with glycosuria being the common parameter measured.25 58 61 Furthermore, only 16 studies extensively reported blood glucose levels of included mice.33 35 38 42 49 59 60 63–65 69 74 77 81 87 91 Only nine studies reported the time required for complete wound healing.18 38 40 52 62 63 80 88 91 Four studies reported measures of wound blood supply,49 69 71 87 with an additional study only reporting perfusion in a subset of mice.29 No investigation reported signs of neuropathy.
The effect of diabetes on wound closure
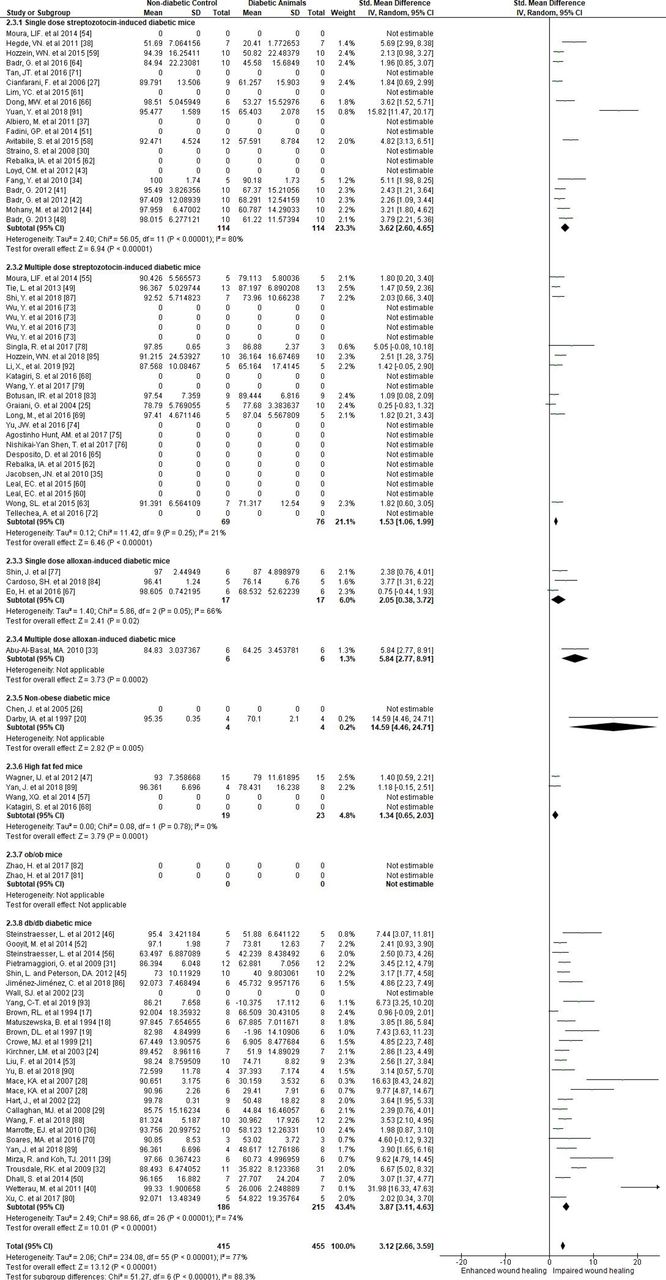
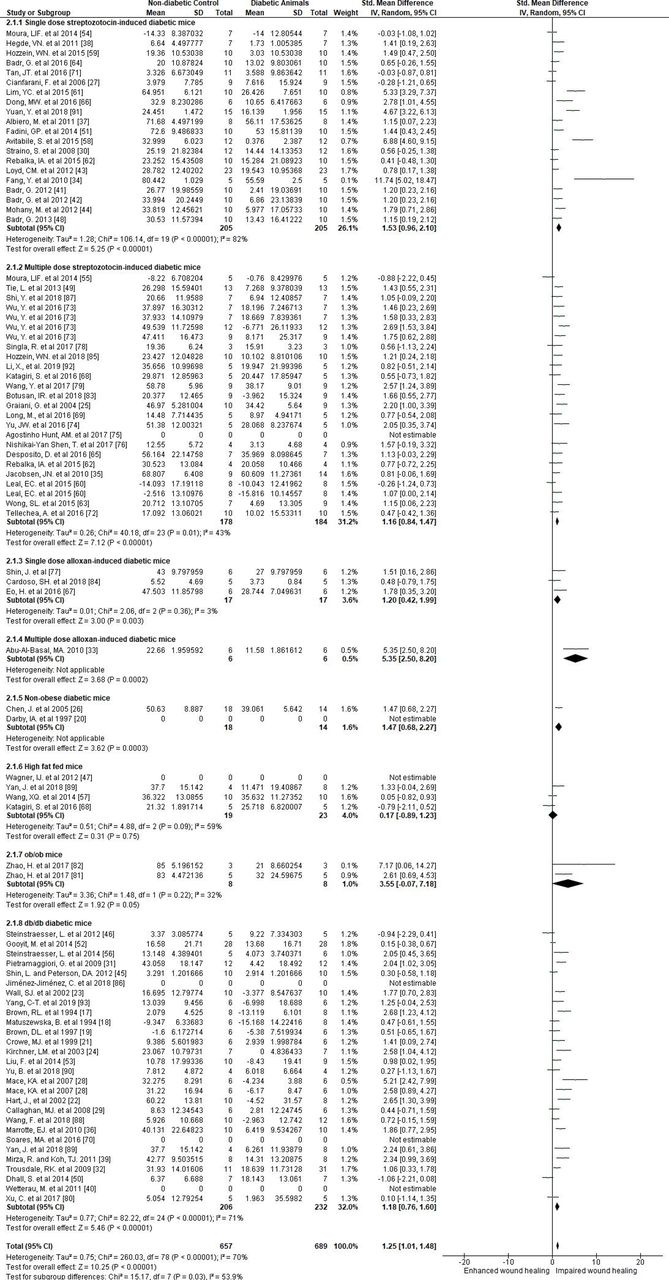
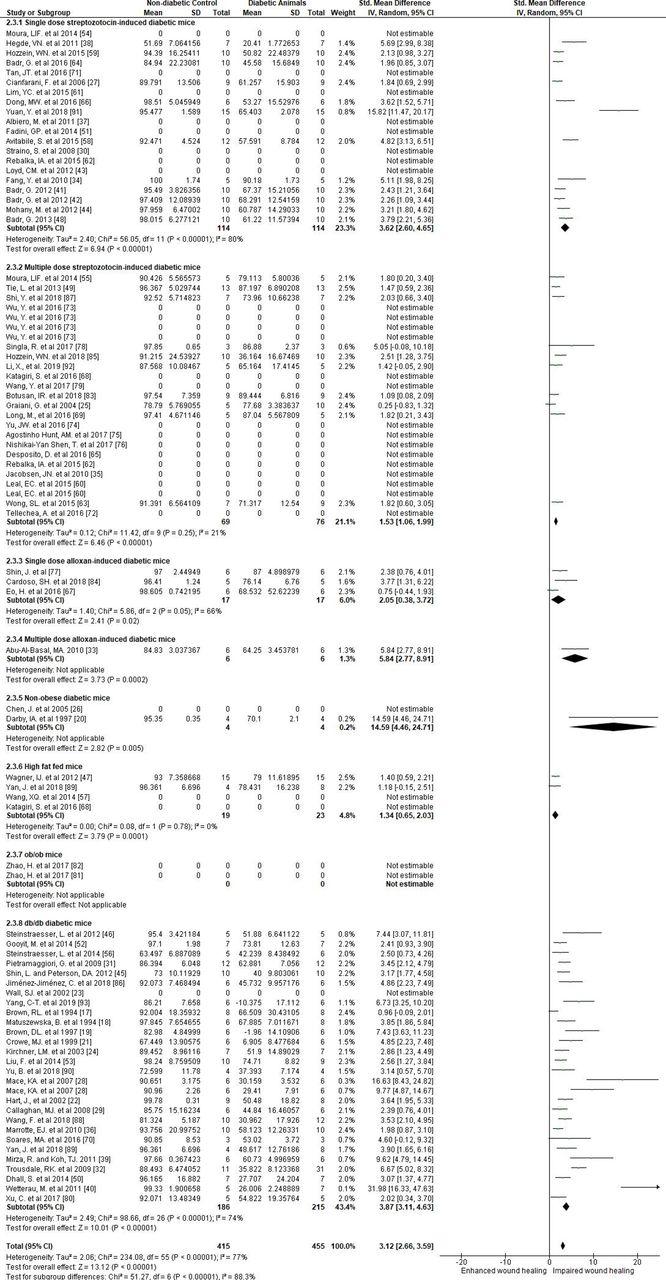
Meta-analyses included data extracted to assess the effect of diabetes on wound closure at early (n=1346), intermediate (n=1398) and late (n=870) stages of wound healing. Diabetes led to impairment of wound closure at all stages (SMD 1.25 (95% CI 1.01 to 1.48, p<0.001), 2.28 (95% CI 1.94 to 2.62, p<0.001) and 3.12 (95% CI 2.66 to 3.59, p<0.001) at early, intermediate and late stages, respectively (figures 1–3 and online supplementary tables 7–9)). There was substantial statistical heterogeneity between studies (I2=70%–80%, figures 1–3 and online supplementary tables 7–9).
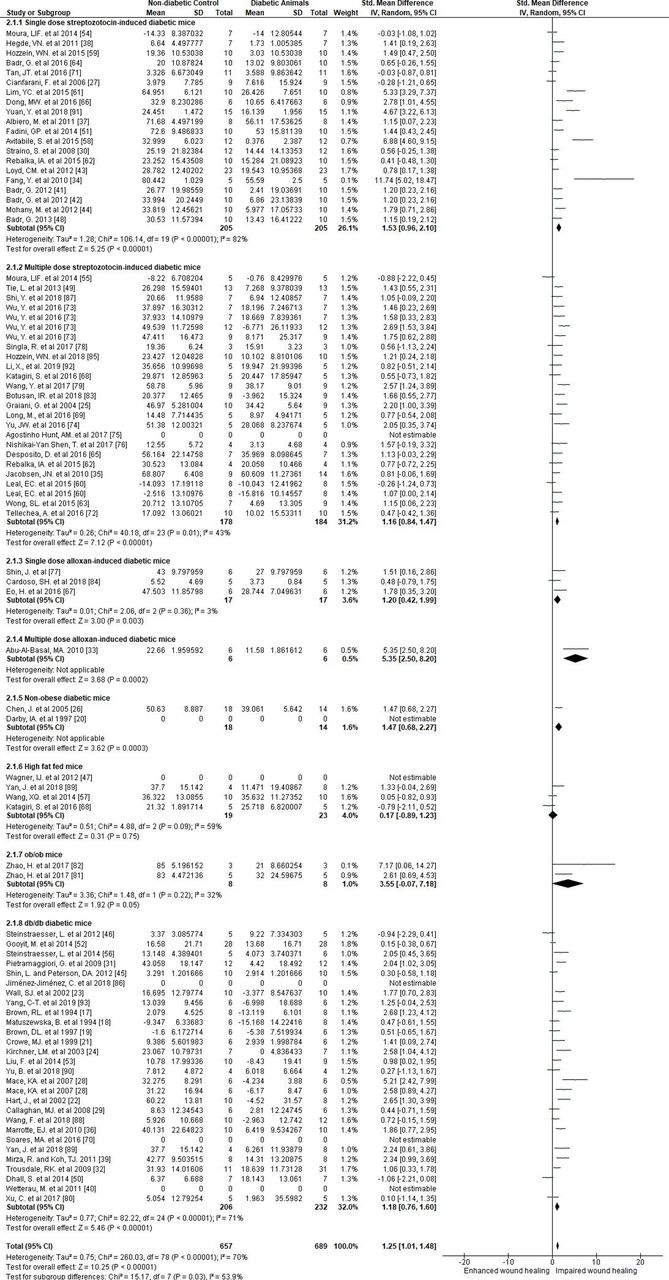
Forest plots showing the effect of diabetes on the early stages of wound closure in different mouse models of diabetes. Forest plots were generated from Review Manager V.5.3 to represent early (2–5 days) stages of wound closure. Comparisons were made using standard mean differences and random effects models.

Forest plots showing the effect of diabetes on the intermediate stages of wound closure in different mouse models of diabetes. Forest plots were generated from Review Manager V.5.3 to represent intermediate (6–10 days) stages of wound closure. Comparisons were made using standard mean differences and random effects models.
{kind=link}
{kind=link}
{kind=link}
Forest plots showing the effect of diabetes on the late stages of wound closure in different mouse models of diabetes. Forest plots were generated from Review Manager V.5.3 to represent late (11–20 days) stages of wound closure. Comparisons were made using standard mean differences and random effects models.
Subgroup analyses suggested that wound closure was significantly impaired when compared with non-diabetic mice at all stages of wound healing in all models of diabetes (figures 1–3 and online supplementary tables 7-9) except in the high-fat fed mice and ob/ob mice at the early stage of wound healing (SMD –0.17 (95% CI −0.89 to 1.23), and SMD 3.55 (95% CI −0.07 to 7.18), respectively) (figure 1 and online supplementary table 7). Pairwise comparisons suggested significant differences in the degree of wound healing impairment in the different diabetes models (online supplementary table 10). db/db mice had greater wound healing impairment than found in the multiple-dose STZ-induced and high-fat fed models at intermediate and late stages of wound healing (online supplementary table 10). The single-dose STZ-induced diabetes model had more severe wound healing impairment than the multiple-dose STZ-induced diabetes model at late stages of wound healing (online supplementary table 10).
Meta-regression suggested that a longer duration of diabetes prior to wound generation was associated with greater impairment of wound healing (online supplementary figure 2c, p=0.021 at late stages after removal of statistical outliers). Leave-one-out sensitivity analyses suggested that all studies contributed towards the main findings in the meta-analysis (online supplementary figure 3). Funnel plots suggested potential publication bias (online supplementary figure 4).
Discussion
This systematic review suggests that mouse models of diabetes consistently have impaired wound healing. The wound healing impairment was clearer as the time after wound induction increased. The severity of wound healing impairment varied between the different mouse models. The meta-regression suggested a tendency towards greater wound healing impairment with longer duration of hyperglycemia. There was substantial statistical heterogeneity and limited reporting of important information in the included studies. Furthermore, very few studies modeled some of the common characteristics of human diabetes-associated ulcers, such as location in the periphery of the limb and concurrent ischemia and neuropathy (online supplementary table 11). These findings highlight the need for more clinically relevant models of diabetes-associated ulceration.
Eight different methods of modeling diabetes were used in the studies included in this systematic review (summarized in table 1, sorted from most to least severe wound healing impairment). Meta-analysis of data reported early after wound induction suggested that the multiple-dose alloxan-induced diabetes model had the most severe wound healing impairment. Meta-analyses of data reported at intermediate and late stages after wound induction suggested that NOD mice had the most severe impairment of wound healing. These findings, however, should be interpreted cautiously given the small and uneven number of studies which reported the use of these models. Indeed, only a total of three studies reported the use of the multiple-dose alloxan-induced diabetes and NOD models. The infrequent use of these models is likely due to a number of factors. First, both models simulate type 1 rather than type 2 diabetes, which is the less common form of diabetes in people.96 Second, these models have disadvantages compared with the more commonly used mouse models of diabetes. For example, alloxan is generally considered less favorable as a diabetogenic agent to STZ due to greater organ toxicity and lower effectiveness,97 while NOD mice have variable onset of diabetes.98 Nonetheless, these models do appear to simulate diabetes-associated wound healing impairment. High-fat feeding is an approach used to simulate type 2 diabetes. This review suggested that this model had the least severe wound healing impairment of all the models examined, possibly due to its milder metabolic derangement. Meta-analyses of data obtained late after wound induction also suggested that impairment of wound healing was more severe in the single-dose STZ-induced diabetes model compared with the multiple-dose STZ-induced diabetes model. It should be noted though that there were substantial methodological differences between the included studies. These comparisons between models should therefore be interpreted very cautiously.
Mouse models of diabetes-associated ulceration ordered in relation to the severity of wound healing impairment
It was surprising to find limited reporting of relevant metabolic parameters and data to confirm the diagnosis of diabetes within the included studies. Susceptibility towards diabetes-associated complications in mice is dependent on a number of different factors, such as age, strain and sex.99–102 Furthermore, studies focusing on other diabetic complications, such as atherosclerosis and neuropathy, typically require an extended duration of diabetes, as well as genetic manipulation, to simulate these complications.9–11 103 104 In the meta-regression, there was a trend towards greater wound healing impairment with longer duration of hyperglycemia before wound induction (online supplementary figure 2). Many of the studies with a relatively long duration of diabetes (>6 weeks) used genetic models which may have influenced the findings of the meta-regression. Nonetheless, investigators should take into consideration the severity and duration of diabetes required to simulate the clinical presentation.
While limbs are the main site of diabetes-associated ulcers in patients, all but three studies included in this systematic review examined wounds generated on the torso of mice. The greater area on the torso allows multiple wounds to be studied but it is unlikely such ulcers simulate the clinical situation. Peripheral artery disease and neuropathy are key causes of ulcers in people. Only four of the included studies examined blood flow within the mice.49 69 71 87 None of the included studies artificially induced artery disease or neuropathy within the mice. Artificial generation of peripheral ischemia or neuropathy is likely required to simulate the clinical presentation since mice are very resistant to development of diabetes-associated microvascular complications.105 Use of genetically modified mice may also be used to simulate other clinically relevant risk factors, such as dyslipidemia which accelerates diabetes-associated atherosclerosis and neuropathy.106 107 Table 2 presents suggested criteria for future diabetes-associated ulcer studies in rodents aimed to improve the clinical relevance of the research.
Proposed reporting standards for mouse models of diabetes-associated ulceration
Limitations and strengths
To the best of our knowledge, this is the first systematic review and meta-analysis examining wound healing impairment in different mouse models of diabetes. The current study used a range of analysis methods and quality assessment methods in order to rigorously assess past research. The included studies had many quality weaknesses such as small sample sizes. There was also absence of key study design and reporting features, like blinding of outcome assessors and inclusion of sample size calculations. Many of the included studies did not report parameters relevant to diabetes or determined the severity of diabetes. Therefore, it was not possible to systematically assess the correlation between glucose control and wound healing impairment. There was also statistical and methodological heterogeneity between studies. Due to the heterogeneous and intermittent reporting of outcomes, it was not possible to systematically examine the molecular mechanisms involved in wound healing impairment. Nonetheless, the findings from this study provide important insight into the strengths and weaknesses of current mice models of diabetes-associated ulcers.
Conclusion
In conclusion, this systematic review suggests that, regardless of diabetes induction method, hyperglycemia impairs wound healing in mice. Incorporation of clinically relevant aspects, such as limb ischemia and prolonged diabetes duration, may improve the translation of findings from the mouse models.
Acknowledgments
We thank Emeritus Professor Rhondda Jones for her statistical advice.
References
Footnotes
Contributors PH, JP, SMK and JG were responsible for the conceptualization of the review, with data curation and analysis performed by PH and JP. The writing of this manuscript was performed by PH and JG.
Funding This work was supported by James Cook University’s Strategic Research Intent Fund. JG holds a National Health and Medical Research Council (NHMRC) Practitioner Fellowship (1117061) and Queensland Government Senior Clinical Research Fellowship (SCRF).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.