Article Text

Abstract
Objective We aimed to study 1-, 5- and 10-year risks of peptic ulcer rebleeding among end-stage renal disease (ESRD) patients with regular haemodialysis, to identify the high-risk subpopulation, and to estimate the number needed to harm (NNH) to increase a peptic ulcer rebleeding in different periods.
Design A nationwide cohort study.
Setting Data from the Taiwan National Health Insurance Research Database.
Patients Uraemic cohort and matched controls were selected from among hospitalised patients with a primary diagnosis of peptic ulcer bleeding. In total, 6447 uraemic patients and 25 788 age-, gender- and gastroprotective agent use-matched controls were selected.
Intervention No.
Main outcome measures Cumulative incidences and HRs.
Results The cumulative incidences of ESRD patients were significantly higher than the cumulative incidences of matched controls (1 year: 18.8% vs 14.2%; 5 years: 38.5% vs 31.4%; and 10 years: 46.3% vs 39.4%; all p<0.001). The NNH to increase a peptic ulcer rebleeding by ESRD at 1, 5 and 10 years were 22, 15 and 15, respectively. On multivariate analysis, ESRD (HR=1.38, p<0.0001) was an independent risk factor for rebleeding. Compared with matched controls, ESRD was associated with higher risk of rebleeding especially in patients using ulcerogenic agents (HR=1.33–1.45), indication to prescribe gastroprotective agents (HR=1.44) and with liver cirrhosis (HR=1.45).
Conclusions ESRD patients had higher long-term risk of peptic ulcer rebleeding, especially in certain populations. The enhanced risk gradually decreased after the first year and stabilised after the fifth year.
- Peptic ulcer
- bleeding
- end-stage renal disease (ESRD)
- cirrhosis
- H. pylori
- non-steroidal anti-inflammatory drugs (NSAIDs)
- bleeding peptic ulcer
- liver cirrhosis
Statistics from Altmetric.com
- Peptic ulcer
- bleeding
- end-stage renal disease (ESRD)
- cirrhosis
- H. pylori
- non-steroidal anti-inflammatory drugs (NSAIDs)
- bleeding peptic ulcer
- liver cirrhosis
Significance of this study
What is already known about his subject?
Although the incidences of peptic ulcer diseases decreased in past decades, peptic ulcer bleeding remains a common medical emergency, especially in patients with co-morbidities.
Patients with ESRD are one of the highest risk populations for short-term risk of peptic ulcer rebleeding.
Liver cirrhosis, Helicobacter pylori infection and the use of non-steroidal anti-inflammatory drugs (NSAIDs) also enhance the risk of peptic ulcer rebleeding.
Gastroprotective agents were underutilised in high-risk populations.
What are the new findings?
ESRD patients had higher 1-, 5- and 10-year risks of peptic ulcer rebleeding. The NNH to increase a peptic ulcer rebleeding by ESRD at 1, 5 and 10 years were 22, 15 and 15, respectively.
On multivariate analysis, ESRD was an independent risk factor for peptic ulcer rebleeding.
Compared with matched controls, ESRD was associated with higher risk of rebleeding especially in patients using ulcerogenic agents, indication to receive gastroprotective agents and with liver cirrhosis.
How might it impact on clinical practice in the foreseeable future?
For ERSR patients with high risk of peptic ulcer rebleeding, long-term PPI or other gastroprotective agents should not be underutilised.
Introduction
Although there have been significant decreases in the incidences of peptic ulcer disease in past decades, peptic ulcer bleeding (PUB) remains a common medical emergency worldwide. In the United States, PUB leads to more than 250 000 admissions annually and costs more than $2.5 billion per year.1 The annual incidence increases with age.1 In Scotland, admission rates for peptic ulcer decreased between 1982 and 2002. However, admission rates for bleeding peptic ulcer increased for subjects aged above 74 years.2 In a Danish study, the incidences decreased 29–33% for uncomplicated peptic ulcers between 1993 and 2002, while the incidence of bleeding ulcer remained stable.3 In Taiwan, we found the incidences of gastric and duodenal ulcer diseases decreased 42–48% and 41–71%, respectively, between 1997 and 2006 in a nationwide cohort study.4 The decreases in incidences were not only observed in uncomplicated peptic ulcer, but also in bleeding peptic ulcers. However, the decreases in incidences among patients older than 80 years were significantly smaller than for the other age groups.4 The increasing proportion of elderly persons in the general population and the associated increases in co-morbidities, especially chronic renal failure, liver cirrhosis, and Helicobacter pylori infection, as well as more frequent use of ulcerogenic agents, such as aspirin or non-steroidal anti-inflammatory drugs (NSAIDs), all enhance the risk of PUB.3–5
Patients with end-stage renal disease (ESRD) are one of the highest risk populations for PUB.6 Several factors contribute to the pathogenesis of higher risk of PUB, including platelet dysfunction, platelet-vessel wall interaction, and blood coagulation abnormalities.7 8 Dialysis and the use of erythropoietin to correct anaemia reduce the incidence of PUB, but do not completely eliminate the risk.9 Although the role of renal failure in increased risk of peptic ulcer rebleeding briefly after admission has been identified,10 11 long-term risk estimation of rebleeding in patients with ESRD and the number needed to harm (NNH) to increase a case of peptic ulcer rebleeding has not been carried out. The influences of age, gender, co-morbidities, H pylori infection, and use of ulcerogenic agents on the long-term risk of peptic ulcer rebleeding also remain unclear.
Patients and methods
Study design
In this population-based cohort study, we recruited patients with ESRD receiving regular haemodialysis admitted due to PUB based on data from Taiwan's National Health Insurance Research Database (NHIRD). The NHIRD consists of healthcare data from nearly the entire Taiwan population of 23.74 million and comprises comprehensive healthcare information, which has been described in detail in our previous studies.5 11 12 This study has been approved by the National Health Research Institutes.
Study population and subjects
Hospitalised patients admitted for the first time between 1 January 1997 and 31 December 2006 with a primary diagnosis of PUB (ICD-9 codes: 531.0, 531.2, 531.4, 531.6, 532.0, 532.2, 532.4, 532.6, 533.0, 533.2, 533.4 and 533.6) were screened. If patients were re-admitted to the same hospital or transferred to another hospital within 3 days of the index hospitalisation, the subsequent admissions were included in the same course of index hospitalisation. Patients <20 years of age and patients who underwent gastric resection or vagotomy before index hospitalisation discharge were excluded. We also excluded patients who developed gastric cancer within the first 2 years of the index hospitalisation as it is difficult to differentiate peptic ulcer from gastric cancer mimicking gastric ulcer.
Uraemic cohort and matched controls
Among the patients with PUB, the uraemic cohort was defined as patients with renal failure diagnosed on previous admission (ICD-9 codes 585 and 586) and receiving regular haemodialysis (more than 9 months) before the index PUB hospitalisation. Patients receiving renal transplantation were excluded. Each patient with uraemia was matched with four controls from the PUB population by age (±2 years), gender and frequency of gastroprotective agent use (0.02% percentage of use of proton pump inhibitors or H2 receptor antagonists). All study subjects were followed up from the index hospitalisation to rehospitalisation for another episode of PUB, death or until the end of 2006.
Outcomes
We analysed the risk of peptic ulcer rebleeding and mortality for the ESRD patients and their matched controls. Rehospitalisation was defined if the study subjects were admitted with a primary diagnosis of PUB following the index hospital discharge for PUB. Cumulative incidences of rebleeding over 1-, 5- and 10-year periods and HRs for these two cohorts were calculated. All-cause mortality within 3 months of rehospitalisation due to PUB was analysed.
To investigate whether the risk associated with the severity of renal failure, we further analysed the cumulative incidences of peptic ulcer rebleeding among patients with different frequency of haemodialysis.
Exposure to ulcerogenic medications and co-morbidities
For all subjects of the two cohorts, ulcerogenic drugs during the whole period of follow-up after the index hospitalisation were analysed, including low-dose and high-dose aspirin, NSAIDs, COX-2 specific inhibitors, and other anti-coagulants (clopidogrel, dipyridamole, warfarin, ticlopidine, cilostazol and cerenin). All information on ulcerogenic drug use by individual patients was obtained from the NHIRD, as this database contains details of every prescription for nearly the entire population of Taiwan, including dose, frequency, starting and ending dates, and administration routes, etc. The frequency of ulcerogenic drug use was defined as average number of days taking these drugs per 30 days within the whole follow-up years. Occasional, frequent and regular users were defined if the study subjects received 1–10 days, 10–19 days and 20–30 days per month, respectively.
Co-morbidities, including previous ischaemic heart disease, cerebral infarction, hypertension, diabetes, chronic obstructive lung disease, liver cirrhosis, and hyperlipidaemia, were defined as diseases diagnosed on admissions before the index hospitalisation and during the period of follow-up.
H pylori-associated peptic ulcer
Hr pylori-associated peptic ulcer was defined as the receiving of H pylori eradication therapy during or after the index hospitalisation. H pylori eradication therapy was defined as proton pump inhibitors or H2 receptor antagonists, plus clarithromycin or metronidazole, plus amoxicillin or tetracycline, with or without bismuth, and other regimes (details of all eligible H pylori eradication regimens are described in our previous studies).11 12
Statistical analysis
Cumulative incidence analyses were conducted using Kaplan–Meier method, and the differences between the curves were calculated with the two-tailed log-rank test. NNH was calculated as the inverse of the attributable risk (the absolute difference between two cohorts compared). Cox proportional hazards model was used to determine whether ESRD is an important risk factor for peptic ulcer rebleeding. We included frequency of ulcerogenic drug use, frequency of gastroprotective agent use, dialysis, H pylori-associated ulcer, and all co-morbidities listed in table 1 in the model analysis. Assessment of goodness-of-fit of the models with the step-down method was used to analyse the independent prognostic factors. All data management and SIR analyses were performed using SAS 9.1 software. Cumulative incidences and HRs were analysed via the SPSS program for Windows 11.0.
Baseline characteristics of uraemic cohort and matched controls
Results
Demographic data
Among the 271 030 subjects who were admitted for the first time with a primary diagnosis of PUB between 1997 and 2006, 6447 were diagnosed with ESRD and 25 788 were selected as controls by matching age, gender and frequency of gastroprotective agent use. Twenty-four male patients with ESRD who could not be matched to male controls due to insufficient numbers were matched to female controls. Other demographic data, including H pylori-associated peptic ulcer, mean follow-up time, frequency of ulcerogenic drug use, frequency of gastroprotective agent use, and co-morbidities, are shown in table 1. Among the uraemic cohorts, only 47 subjects received peritoneal haemodialysis. The median, 25% and 75% quartiles of frequency of dialysis for the uraemic cohort was 2.98, 0.94 and 3.28 times per week, respectively.
Cumulative incidences of peptic ulcer rebleeding and mortality
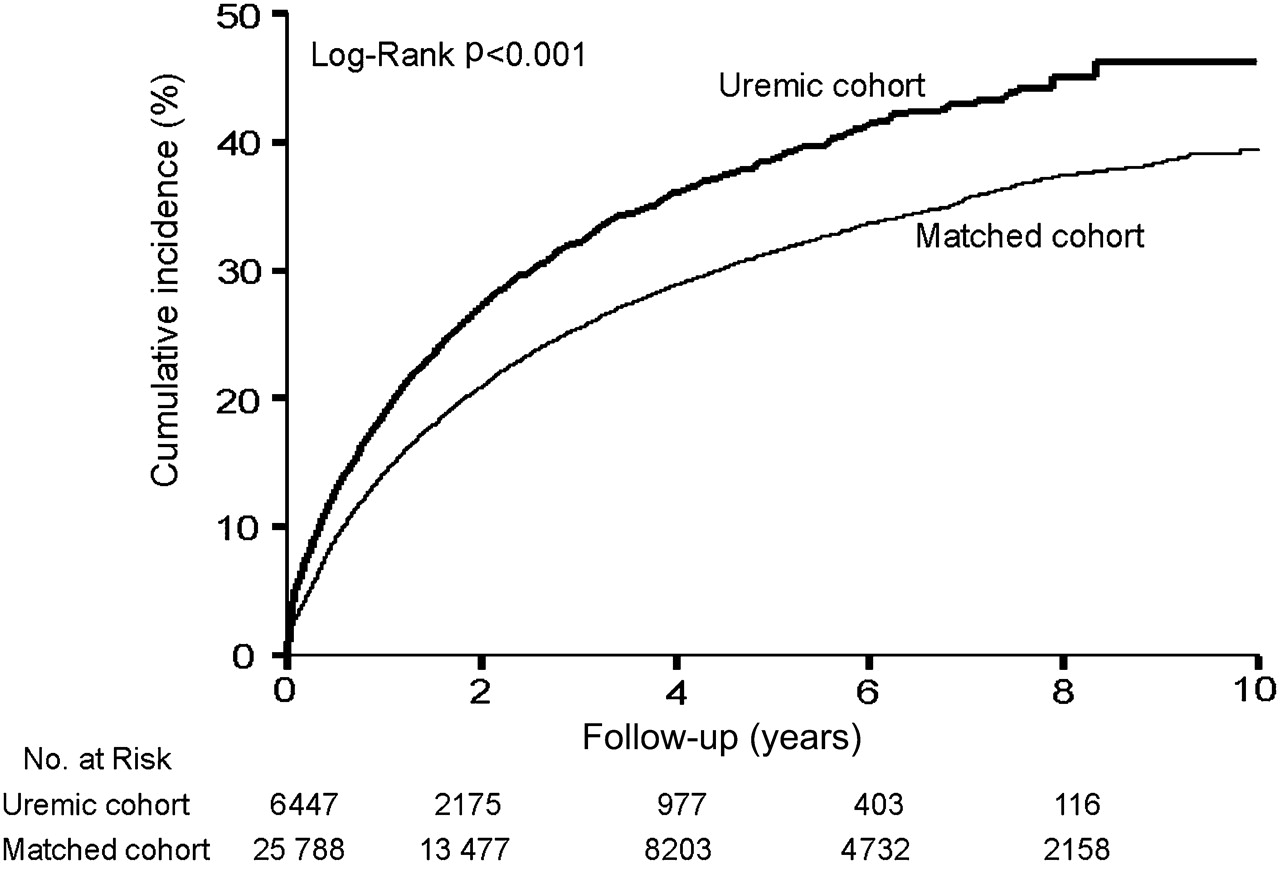
The 1-year cumulative incidence of peptic ulcer rebleeding in patients with ESRD was significantly higher than the 1-year cumulative incidence of controls (18.8% vs 14.2%, p<0.001). The 5-year and 10-year cumulative incidences of peptic ulcer rebleeding in patients with ESRD were also significantly higher than the 5-year and 10-year cumulative incidences of matched controls (5 years: 38.5% vs 31.4%, p<0.0001; 10 years: 46.3% vs 39.4%, p<0.001) (figure 1). The numbers needed to increase a case of peptic ulcer rebleeding by ESRD (NNH) for 1, 5 and 10 years were 22, 15 and 15, respectively. Patients receiving haemodialysis fewer than three times per week had a slightly, but not significantly lower risk of peptic ulcer rebleeding compared with those receiving haemodialysis equal or more than three times per week (p=0.9068) (Supplemental figure 1).

Cumulative incidences of peptic ulcer rebleeding for uraemic cohort and age-, gender- and gastroprotective agent-matched controls.
The cumulative incidences of rebleeding within 7 days were 1.7% and 1.0% for patients with ERSD and matched controls, respectively (p<0.001) (Supplemental figure 2A). The cumulative incidences of rebleeding in the first 30 days after discharge were 5.0% and 2.7% for patients with uraemia and controls, respectively (Supplemental figure 2B).
The 1-, 5- and 10-year cumulative incidences of mortality in patients with ESRD were significantly higher than the 1-, 5- and 10-year cumulative mortality incidences of controls (1 year: 3.5% vs 1.4%, p<0.0001; 5 year: 7.0% vs 2.8%, p<0.0001; 10 years: 9.0% vs 3.9%, p<0.0001) (figure 2).

Cumulative incidences of all-cause mortality within 3 months of rehospitalisation due to peptic ulcer bleeding.
The 10-year cumulative incidences of rebleeding according to H pylori and NSAIDs status for both cohorts were as follows: H pylori associated (ESRD vs controls: 53.8% vs 44.8%, p<0.0002), non-H pylori-associated (ESRD vs controls: 45.0% vs 37.4%, p<0.0001), NSAID associated (ESRD vs controls: 48.0% vs 36.1%, p<0.0001) and non-NSAID associated (ESRD vs controls: 41.2% vs 45.5%, p=0.4416).
For patients with cirrhosis, the 10-year cumulative incidences of peptic ulcer rebleeding were 55.1% and 47.8% for patients with ESRD and for controls, respectively (p<0.0001). The 10-year cumulative incidences of variceal bleeding were 24.1% and 22.3% for patients with uraemia and the matched controls, respectively.
Relative risk of peptic ulcer rebleeding
On Cox multivariate proportional hazards analysis, ESRD (HR=1.38, p<0.0001), ulcerogenic drugs (HR=1.03 for each 10% incremental use in frequency, p<0.0001), H pylori-associated peptic ulcer (HR=1.19, p<0.0001), and co-morbidities with past history of liver cirrhosis (HR=1.44, p<0.0001) were independent risk factors for peptic ulcer rebleeding (table 2).
Multivariate Cox proportional hazards model analysis for prediction of peptic ulcer rebleeding
We further analysed the data to examine the immediate effect of ulcerogenic drugs use within 14 days before the end time of the observation period. We found each one incremental day use of an ulcerogenic agent increased 6% risk of peptic ulcer rebleeding (table 3).
Multivariate Cox proportional hazards model analysis for prediction of peptic ulcer rebleeding (ulcerogenic drugs within 14 days before the end time)
Multivariate stratified analysis
Figure 3 shows the results of multivariate stratified analysis. In each stratum, the HRs were compared between patients with uraemia and the matched cohort subjects. For the 20–49, 50–59, 60–69 and ≥70 age groups, ESRD was associated with significantly higher risks of peptic ulcer rebleeding compared with the matched controls (HR=1.71, 1.37, 1.55 and 1.24, respectively). For males and females, ESRD was associated with similar risks of rebleeding. For patients with indications to receive gastroprotective agents, ESRD had higher risk of rebleeding than controls (HR=1.44). For patients not receiving ulcerogenic agents, ESRD was not associated with a higher risk of rebleeding. For those receiving occasional, frequent or regular ulcerogenic agents, higher risks of rebleeding were found in the patients with ESRD (HR=1.45, 1.33, and 1.38, respectively). For patients with liver cirrhosis, ESRD was associated with a higher risk of rebleeding (HR=1.45).

{kind=link}
{kind=link}
{kind=link}
Multivariate stratified analysis: HRs for end-stage renal disease in subgroups of patients after adjusting for all other factors. In each stratum, the HRs were compared between end-stage renal disease patients and the matched cohort subjects.
Discussion
Although the role of ESRD in short-term peptic ulcer rebleeding risk has been investigated, our study is the first to analyse the role of ESRD in the 10-year risk of peptic ulcer rebleeding and mortality. ESRD is found to be associated with a significantly higher risk of peptic ulcer rebleeding and mortality starting from the beginning of discharge from the index hospitalisation and persisting for 10 years. The enhanced risk gradually decreases from the first year and stabilises after 5 years. NNH remains stable between 5 years and 10 years.
ESRD and liver cirrhosis were found to be the most significant risk factors for peptic ulcer rebleeding. The impact of these co-morbidities was even higher than the influences of age, gender, status of H pylori infection, and use of ulcerogenic agents. Our observations are compatible with previous reports regarding short-term risk of peptic ulcer rebleeding. Rockall et al reported that renal failure and liver failure were the highest predictors of peptic ulcer mortality and rebleeding.10 Blatchford et al found liver disease predicted higher risk of rebleeding.13 In a recent study, liver cirrhosis was found to be one of the major risk factors related to peptic ulcer rebleeding.14 On stratified analysis, we found ESRD had significantly higher risk of peptic ulcer rebleeding in patients with cirrhosis.
Meta-analysis has approved that H pylori eradication is effective in preventing peptic ulcer rebleeding;15 however, a recent study by Wong et al found peptic ulcer rebleeding and mortality rates were higher in patients with neither H pylori nor NSAIDs bleeding ulcers.16 These observations were actually consistent in considering the different aetiologies of PUB. For those with H pylori-negative idiopathic bleeding ulcers, co-morbidities may be the major reason of bleeding and contribute to the following rebleeding and mortality. For H. pylori-infected patients, eradication therapy eliminates the pathogen and reduces the risk of rebleeding. In the present study, we defined H pylori associated peptic ulcer as the receiving of H pylori eradication therapy during or after the index hospitalisation. Since the time of H pylori eradication was likely to be close to the first episode of bleeding, rebleeding events 5–10 years after H pylori eradication should not be considered to be H pylori associated. However, rebleeding events shortly after the index hospitalisation may still be increased by H pylori infection. Compared with the H pylori and NSAID-negative patients reported by Wong et al, the rebleeding rates in both ESRD patients and controls in the present study were similar.16 However, the overall mortalities in the present study were much lower because we only analysed morality within 3 months of rehospitalisation due to PUB, in contrast to mortality at any time point reported by Wong et al.
Use of ulcerogenic agents was found to be an independent risk factor for rebleeding. In addition, we did not find a dose-dependent response pattern. Instead, the change in the impact of ESRD on peptic ulcer rebleeding was more dramatic. Once patients used ulcerogenic agents, the risk of peptic ulcer rebleeding increased no matter whether the use of these ulcerogenic agents was occasional, frequent or regular. Despite the fact that most guidelines recommend gastroprotection in high-risk patients, under-utilisation of gastroprotective agents has been reported in many studies.17–19 In the USA, more than 80% of patients receiving aspirin after percutaneous coronary intervention missed their proton pump inhibitor (PPI) co-therapy initiation.17 In Canada, 44% of aspirin users with a history of peptic ulcer complications did not receive concomitant PPI therapy.18 In France, only half of NSAID users above 65 years received gastroprotective agents.19 Our observations provide important evidence to avoid under-utilisation of gastroprotective agents in high-risk patients receiving NSAIDs.
In the present study, it was not clear whether the higher risk of rebleeding was bleeding from the same ulcer or recurrent but a new ulcer. It was also unclear whether the increase in rebleeding rate was related to the increased use of heparin or anti-coagulant for dialysis or was related to the ESRD. We could only hypothesise that if it was related to the anticoagulants used, the recurrent bleeding was more likely to arise from the same ulcer and rebled earlier. In Supplemental figure 2, we found 7-day and 30-day cumulative incidences of rebleeding for uraemic cohorts were 1.7% and 5.0%, respectively. If recurrent bleeding occurred 1 month thereafter could be defined as new ulcers, most rebleeding events in the present study were related to ESRD instead of anticoagulants use. Using long-term PPI or gastroprotective agents as secondary prevention could be substantiated.
In Taiwan, the prescription of PPIs or H2RAs is strictly limited to patients who have had active or healing peptic ulcers confirmed by gastroendoscopy in the past 4 months. Once a peptic ulcer has healed, gastroprotective agents are not paid for by national health insurance and prescription orders cannot be found in the NHIRD. Therefore, the use of PPIs or H2RAs was actually an indicator of prescriptions for gastroprotective agents to treat active or healing ulcers. To prevent the use of a gastroprotective agent as a significant confounder, we matched controls not only by age and gender, but also by the frequency of use of gastroprotective agents.
There are several limitations to the present study. First, we did not have endoscopic findings, which are widely used to predict peptic ulcer rebleeding, including active bleeding, visible vessels, and adherent clots.20 21 However, most of these parameters play important roles briefly after PUB, but not in the long term. Second, our results were based on a retrospective cohort study. Although we matched the controls to balance the demographic characteristics of the study cohorts and conducted multivariate analysis, as well as stratified analysis, to confirm the robustness of our results, unmeasured confounders that affect both groups may exist. In addition, the multiple comparisons conducted may lead to some unexpected results hard to explain, such as ischaemic heart disease as an independent protective factor. Third, H pylori-associated peptic ulcer was defined as the receiving of H pylori eradication therapy in the present study. Based on the insurance database, it is impossible to confirm whether a patient was still infected and whether the rebleeding was due to H pylori-associated peptic ulcer. For those not receiving H pylori eradication therapy, the status of H pylori infection was unknown. It contributed to the large percentages of non-H pylori ulcers in both cohorts. Fourth, self-funded ulcerogenic agents could not be identified in the NHIRD, which tended to underestimate the prevalence of ulcerogenic users. However, the underestimation may only weaken the association, but not bias the results. Finally, we cannot confirm the underlying diseases causing the ESRD in the NHIRD to investigate whether rebleeding risks were altered by different aetiologies of ESRD.
In conclusion, patients with ESRD had a significantly higher long-term risk of peptic ulcer rebleeding. The increased risk was observed on subgroup analysis regardless of patient age, gender, use of gastroprotective agents or ulcerogenic drugs, H pylori status or co-morbidities.
References
Supplementary materials
{kind=link}
{kind=link}
{kind=link}
Footnotes
C-Y Wu and J-T Lin contributed equally to this work as corresponding authors.
Funding This work was supported by the National Health Research Institutes of Taiwan (grant numbers: PH-099-PP-26 and PH-099-PP-16).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.