Article Text

Abstract
Objectives We conducted a systematic literature review and meta-analysis of observational studies to investigate the association between diabetes, hypertension, body mass index (BMI) or smoking with the risk of death in patients with COVID-19 and to estimate the proportion of deaths attributable to these conditions.
Methods Relevant observational studies were identified by searches in the PubMed, Cochrane library and Embase databases through 14 November 2020. Random-effects models were used to estimate summary relative risks (SRRs) and 95% CIs. Certainty of evidence was assessed using the Cochrane methods and the Grading of Recommendations, Assessment, Development and Evaluations framework.
Results A total of 186 studies representing 210 447 deaths among 1 304 587 patients with COVID-19 were included in this analysis. The SRR for death in patients with COVID-19 was 1.54 (95% CI 1.44 to 1.64, I2=92%, n=145, low certainty) for diabetes and 1.42 (95% CI 1.30 to 1.54, I2=90%, n=127, low certainty) for hypertension compared with patients without each of these comorbidities. Regarding obesity, the SSR was 1.45 (95% CI 1.31 to 1.61, I2=91%, n=54, high certainty) for patients with BMI ≥30 kg/m2 compared with those with BMI <30 kg/m2 and 1.12 (95% CI 1.07 to 1.17, I2=68%, n=25) per 5 kg/m2 increase in BMI. There was evidence of a J-shaped non-linear dose–response relationship between BMI and mortality from COVID-19, with the nadir of the curve at a BMI of around 22–24, and a 1.5–2-fold increase in COVID-19 mortality with extreme obesity (BMI of 40–45). The SRR was 1.28 (95% CI 1.17 to 1.40, I2=74%, n=28, low certainty) for ever, 1.29 (95% CI 1.03 to 1.62, I2=84%, n=19) for current and 1.25 (95% CI 1.11 to 1.42, I2=75%, n=14) for former smokers compared with never smokers. The absolute risk of COVID-19 death was increased by 14%, 11%, 12% and 7% for diabetes, hypertension, obesity and smoking, respectively. The proportion of deaths attributable to diabetes, hypertension, obesity and smoking was 8%, 7%, 11% and 2%, respectively.
Conclusion Our findings suggest that diabetes, hypertension, obesity and smoking were associated with higher COVID-19 mortality, contributing to nearly 30% of COVID-19 deaths.
Trial registration number CRD42020218115.
- COVID-19
- hypertension
- general diabetes
- epidemiology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We did a systematic review and meta-analysis of 186 observational studies (210 447 deaths among 1 304 587 patients with COVID-19) to investigate the association between diabetes, hypertension, obesity and smoking and risk of death in patients with COVID-19 and to estimate the proportion of deaths attributable to these four conditions.
We performed several subgroup analyses, and assessed certainty of evidence using the Cochrane methods and the Grading of Recommendations, Assessment, Development and Evaluations framework. A non-linear dose–response relation between body mass index and COVID-19 mortality was also explored.
However, we did not investigate the association between presence of two or more coexisting comorbidities and risk of death in patients with COVID-19.
Introduction
COVID-19 is a viral infectious disease caused by SARS-CoV-2, which was first reported in Wuhan City, China, in December 2019.1 SARS-CoV-2 has since spread to all countries worldwide and COVID-19 has been declared a pandemic by the WHO.2 As of 24 August 2021, over 212.3 million cases and 4.4 million deaths have been reported globally since the start of the pandemic.3 Age is the main risk factor for poor outcome in people with COVID-19 infection,4 5 as it is correlated with more comorbidities. About 70%–87% of COVID-19 deaths are among people aged 70 years or older.6 7 Patients with comorbidities, including diabetes, cardiovascular disease, respiratory disease, chronic kidney disease and others chronic diseases are at increased risk of developing severe or critical COVID-19,8 9 which may partly explain a greater mortality in hospital.10–14 Studies suggest that about 20%–51% of patients hospitalised with COVID-19 have at least one comorbidity.10 15
Previous meta-analyses reported a higher mortality rate from COVID-19 in patients with comorbidities.16–22 Ssentongo et al, based on 25 studies published from December 2019 to 9 July 2020, suggested that diabetes and hypertension were respectively associated with a 1.48-fold and 1.82-fold greater risk of COVID-19 death compared with those without these comorbidities.16 Based on studies published during the same period, Luo et al reported similar results.17 Du et al found that patients with obesity had a 2.68-fold risk of dying from COVID-19 compared with non-obese patients.18 Most of the published meta-analyses did not investigate the shape of the dose–response relationship between body mass index (BMI) and risk of death in order to clarify whether the association is dose-dependent or if there are threshold effects.20 23–25 In addition, evidence suggests that smoking may increase risk of severe disease and death from COVID-19.19 However, it is not clear whether such an increase in COVID-19 mortality is different in current and past smokers since previous meta-analyses have not performed separate analyses.19 26 27
However, since the publication of these meta-analyses, several observational studies have been published on diabetes, hypertension, obesity or smoking and risk of death in patients with COVID-194 28–122 and the strength of the associations differed greatly between studies. Moreover, the proportion of deaths attributable to diabetes, hypertension, obesity or smoking habits has not been estimated. This last aspect may help adapting public health measures and vaccination strategies to populations at risk of severe COVID-19.
Given the rapidly increasing death from COVID-19 globally, and since diabetes, hypertension, obesity and tobacco smoking represent the most important public health problems worldwide, which contributed to higher risk of death globally; we thus conducted a systematic review and meta-analysis of published observational studies to investigate the association between diabetes, hypertension, smoking and obesity and risk of death in patient with COVID-19 and to clarify the strength of these associations. We further estimated the proportion of deaths attributable to these conditions.
Materials and methods
Search strategy and selection criteria
The meta-analysis was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement123 and Meta-Analysis of Observational Studies in Epidemiology.124 This study was registered and accepted in the International Prospective Register of PROSPERO in October 2020. PubMed (MEDLINE), Cochrane library and Embase databases were searched to identify relevant articles published in English from December 2019 to 14 November 2020. The search terms that we used are provided in online supplemental file. In addition, we searched the reference lists of the relevant publications, reviews and meta-analyses to identify additional potentially relevant studies. We only included observational studies (cohort studies and cross-sectional) that reported relative risk estimates (such as hazard ratios (HRs), relative risk (RR) or odds ratios (ORs)) with the 95% CIs with or without adjustment for potential confounders. The search was independently screened by two researchers (YM-S and TF) and discrepancies were resolved by discussion with a third researcher (MER).
Supplemental material
Data collection
From each included publication, we extracted results and study characteristics which included first author’s last name, publication year, country where the research was conducted in, study design, study description or name, study period, sample size with number of deaths, exposure, categories, risk estimate and 95% CIs, and adjustment factors. Data were extracted by YM-S and extractions were checked for accuracy by TF. Discrepancies were resolved through discussion with a third researcher (MER).
Quality assessment and risk of bias
The quality of individual studies was assessed independently by two researchers (YM-S and TF) using the Cochrane risk of bias tool ROBINS-I, which grades studies on a scale from critical risk of bias to low risk of bias considering bias due to confounding, selection of study participants, exposure measurement, misclassification of exposure during follow-up, missing data, measurement of outcomes and bias due to selection of reported results.125 Following the assessment of risk of bias, the body of evidence for each comorbidity and risk of death was rated independently using the Grading of Recommendations, Assessment, Development and Evaluations approach.126 Discrepancies were resolved through discussion with a third researcher (DA).
Data analysis
We used random effects models that consider both within study and between-study variation to calculate summary RRs (SRRs) (95% CIs) of COVID-19 mortality for patients with diabetes compared with those without diabetes, for patients with hypertension versus those without hypertension, for obese versus non-obese and for current, former and ever smoker compared with never smokers. The natural logarithm of the RRs was weighted using random effects weights.127 Statistical heterogeneity between studies was assessed by the Cochrane Q test and the I2 statistic.128 We calculated the absolute risk difference (RD) from the baseline risk of mortality (BR) from Docherty et al,129 large cohort and relative risk (RR) using the formula RD=BR×(RR−1).130
We further performed a dose–response analysis for the associations between BMI and COVID-19 mortality using the method described by Greenland and Longnecker to compute the linear trend from the natural logs of the RRs and CIs across categories of BMI.131 We calculated SRRs and 95% CIs for a 5-unit increment in BMI using random effects models. This method required mean or median of BMI, RRs and 95% CIs for at least three categories. The mean or median BMI level per category was used if provided in the publication, and if not, the midpoint of the upper and lower boundaries was estimated as a range in each category. When the highest and lowest categories were open-ended, we used the width of the adjacent interval to estimate the upper and lower boundaries for the category. For studies that reported results separately for young and adults, for current and former smoker, but not overall, we pooled the results using a fixed-effects model as reported by the Hamling procedure to obtain an overall estimate to be used in the meta-analysis.132
To explore the potential non-linear dose–response relation between BMI and mortality among patients with COVID-19, we used fractional polynomial models.133 We determined the best fitting second order fractional polynomial regression model, defined as the one with the lowest deviance. Only studies which presented more than two categories of BMI were included in the non-linear analysis. Subgroup and meta-regression analyses were conducted to investigate potential sources of heterogeneity. Small-study effects, such as publication bias, were visually assessed by examining funnel plots for asymmetry, and with Egger’s test,134 and the results were considered to indicate potential small-study bias when p values were <0.10. We conducted sensitivity analyses excluding one study at a time to clarify whether the results were driven by one large study or a study with an extreme result.
We finally calculated the population attributable fraction (PAF) of mortality among patients with COVID-19 due to diabetes, hypertension, obesity and smoking, worldwide using the following formula135:

Where RR was the relative risk, p was the prevalence of the exposure in patient with COVID-19. The prevalence of diabetes (11.5%), hypertension (22.9%), obesity (29%) and smoking (9%) were obtained from previous meta-analyses.136–138
Patient and public involvement
Patients or the public were not involved in any aspect of the study design, conduct or in the development of the research question or outcome measures.
Results
A total of 6007 records were identified in MEDLINE, Cochrane library and in EMBASE (figure 1). A total of 4665 publications were excluded after reading title and abstract or because of duplicates. Among 1342 full-text articles retrieved, 994 were excluded as not meeting the inclusion criteria, leaving a total of 348 publications. Of these, 162 articles were not eligible because they lacked sufficient data,139 140 reported no risk estimate or irrelevant data,139 140 because they had identical populations141–151 or were retracted.152 Finally, a total of 186 observational studies were included in this meta-analysis. Of the included studies, 58 were from Europe, 58 from North America, 60 from Asia, 6 from South America and 4 from Africa (online supplemental table 1). From the 186 publications assessed using the ROBINS-I tool, 92 were evaluated as being at low risk of bias, 49 at moderate risk of bias, 21 at serious risk of bias and 24 at critical risk of bias because of insufficient adjustment of relevant confounders (online supplemental table 2).

Flow-chart of study selection.
Diabetes and mortality in patient with COVID-19
A total of 145 studies4 28–119 121 122 129 153–201 were included in the analysis of the association between diabetes and mortality, including a total of 198 491 deaths among 1 165 897 patients with COVID-19. The SRR for diabetes patients compared with those without diabetes was 1.54 (95% CI 1.44 to 1.64) and there was high heterogeneity among studies (I2=92%). We found that diabetes increased the absolute risk of death by 14% (table 1). The funnel plot did not provide evidence of publication bias (online supplemental figure 1) and we found no evidence of small study effects (Egger’s test, p value=0.54).
Supplemental material
Summary relative risk, risk difference and fraction of deaths attributable to diabetes, hypertension, obesity and smoking in patients with COVID-19
The positive association persisted across all subgroups analyses stratified by study design, number of patients, geographic location and adjustment for some confounding factors (table 2). However, meta-regression analyses suggested some indication of heterogeneity between studies that adjusted for multiple factors such as age, sex and other comorbidities versus studies without such adjustment or adjusted for age only (Pheterogeneity=0.003), with a stronger association for the studies with no adjustment factors or those adjusted for age only. The positive association was also stronger among studies with critical or serious risk of bias compared with those with moderate or low risk of bias, with heterogeneity detected across studies (Pheterogeneity=0.001).
Subgroup analyses of association between diabetes and hypertension and mortality risk in patients with COVID-19
The influence analysis showed no substantial influence of any of the included studies on the global estimate of diabetes and mortality. The SRR ranged from 1.51 (95% CI 1.42 to 1.61) when excluding the Barbu et al study35 to 1.55 (95% CI 1.45 to 1.64) when excluding the Meng et al study114 (online supplemental figure 2).
Association between obesity and mortality risk in patients with COVID-19.
Hypertension and mortality in patient with COVID-19
We included 127 observational studies4 29 30 32 33 35–40 42–45 47–50 52–56 58 59 61–63 65 66 69 71–76 78 81–84 86 88–90 92–95 97 103 105 106 108–112 114–118 120–122 153 154 156–159 161–167 169 173–180 182–188 193–200 202–219 in the analysis of the association between hypertension and mortality, including a total of 113 243 deaths among 934 958 patients with COVID-19. The SRR for hypertension patients versus those without hypertension was 1.42 (95% CI 1.30 to 1.54) with high evidence of heterogeneity (I²=90%) (table 1). The absolute risk of death for patients with COVID-19 with hypertension compared with without hypertension was increased by 11%. Small study effects, such as publication bias, were not indicated with the funnel plot (online supplemental figure 3) or Egger’s test (p value=0.26).

Association between body mass index (BMI) and mortality risk in patients with COVID-19, linear dose–response analysis, per 5 kg/m2 increment of BMI.
Here again, the positive association persisted in most subgroup analyses (table 2). Our meta-regression analysis showed that the study design and the geographic location did not significantly influence the magnitude of the overall association. However, heterogeneity between subgroup analyses was observed in analyses stratified by risk of bias with higher association for studies with critical compared with those with low, moderate or serious risk of bias (Pheterogeneity≤0.0001) and by adjustment for confounding factors with higher association for studies without adjustment compared with those that adjusted for age only or for multiple factors (Pheterogeneity≤0.0001).
When excluding the most influential studies, we found no substantial influence of any of the included studies (online supplemental figure 4).

Association between body mass index (BMI) and mortality risk in patients with COVID-19: non-linear dose–response analysis.
BMI and mortality in patient with COVID-19
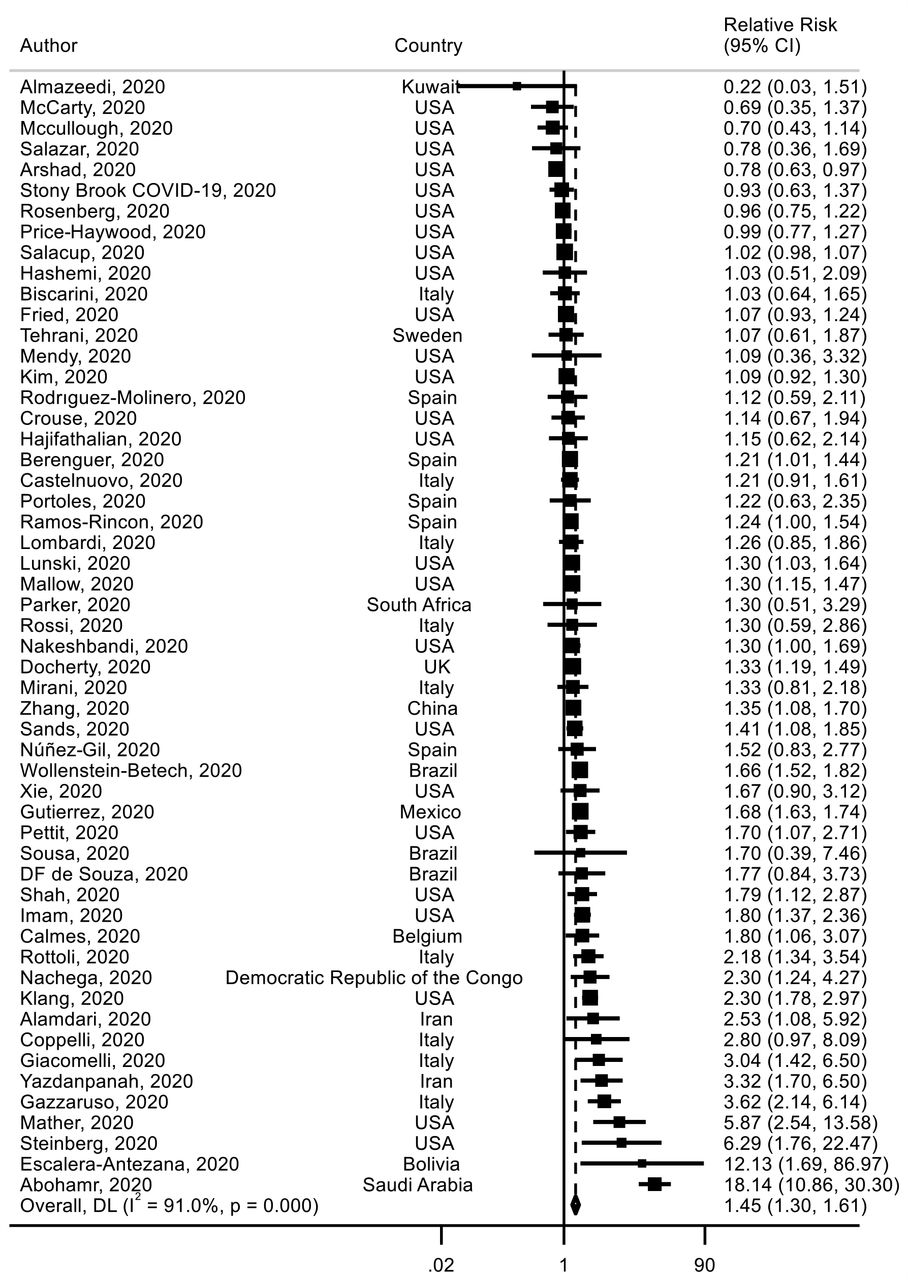
Fifty-four studies29 32 38 44 45 48 49 52 61 62 64 65 67 69 73 74 79 84–86 88–90 93 99 103 107 118 120–122 129 154 164 165 178 181 182 184 192 196 197 202 206 220–228 investigated BMI and mortality risk including 145 605 deaths among 858 374 patients with COVID-19 were identified. The analysis yielded an SRR of 1.45 (95% CI 1.31 to 1.61) for obese (BMI ≥30 kg/m2) versus non-obese (BMI <30 kg/m2) patients, with high heterogeneity detected between studies (I²=91%) (figure 2) (table 1). We found that obesity increased the absolute risk of death by 12%. There was no statistically significant evidence of publication bias (p value Egger’s test=0.92) (online supplemental figure 5). The meta-regression analysis showed that study characteristics did not significantly alter the overall estimate (online supplemental table 3). When excluding the most influential studies one by one, the global estimate did not substantially change (online supplemental figure 6).

Association between ever smoking (vs never smoking) and mortality risk in patients with COVID-19.
Association between current smoking (vs never smoking) and mortality risk in patients with COVID-19.
Twenty-five studies (32 072 deaths among 95 852 patients with COVID-19)38 56 61 74 86 89 91–93 97 108 111 112 161 162 175 177 221 222 229–235 were included in the dose–response meta-analysis of BMI and mortality risk. The summary RR for a 5 kg/m2 increment in BMI was 1.12 (95% CI 1.07 to 1.17, I2=68%) (figure 3) and no statistically significant evidence of publication bias (p value=0.11) or by inspection of the funnel plot was observed (online supplemental figure 7). However, evidence of a J-shaped non-linear relation between BMI and mortality risk was observed (Pnon-linearity≤0.0001), suggesting a flat dose–response curve at a BMI around 22–24 kg/m2 with a slight increase in risk of death below that range and a 1.5–2-fold increase in risk of death with a BMI of 40–45 versus 22–24 kg/m2 (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association between former smoking (vs never smoking) and mortality risk in patients with COVID-19.
In sensitivity analyses excluding one study at a time from the analysis, the summary for a 5 kg/m2 increment in BMI ranged from 1.11 (95% CI 1.06 to 1.15) when excluding the Czernichow et al. Study108 to 1.13 (95% CI 1.08 to 1.19) when excluding the Ferrando-Vivas et al study230 (online supplemental figure 8).
Smoking and mortality in patient with COVID-19
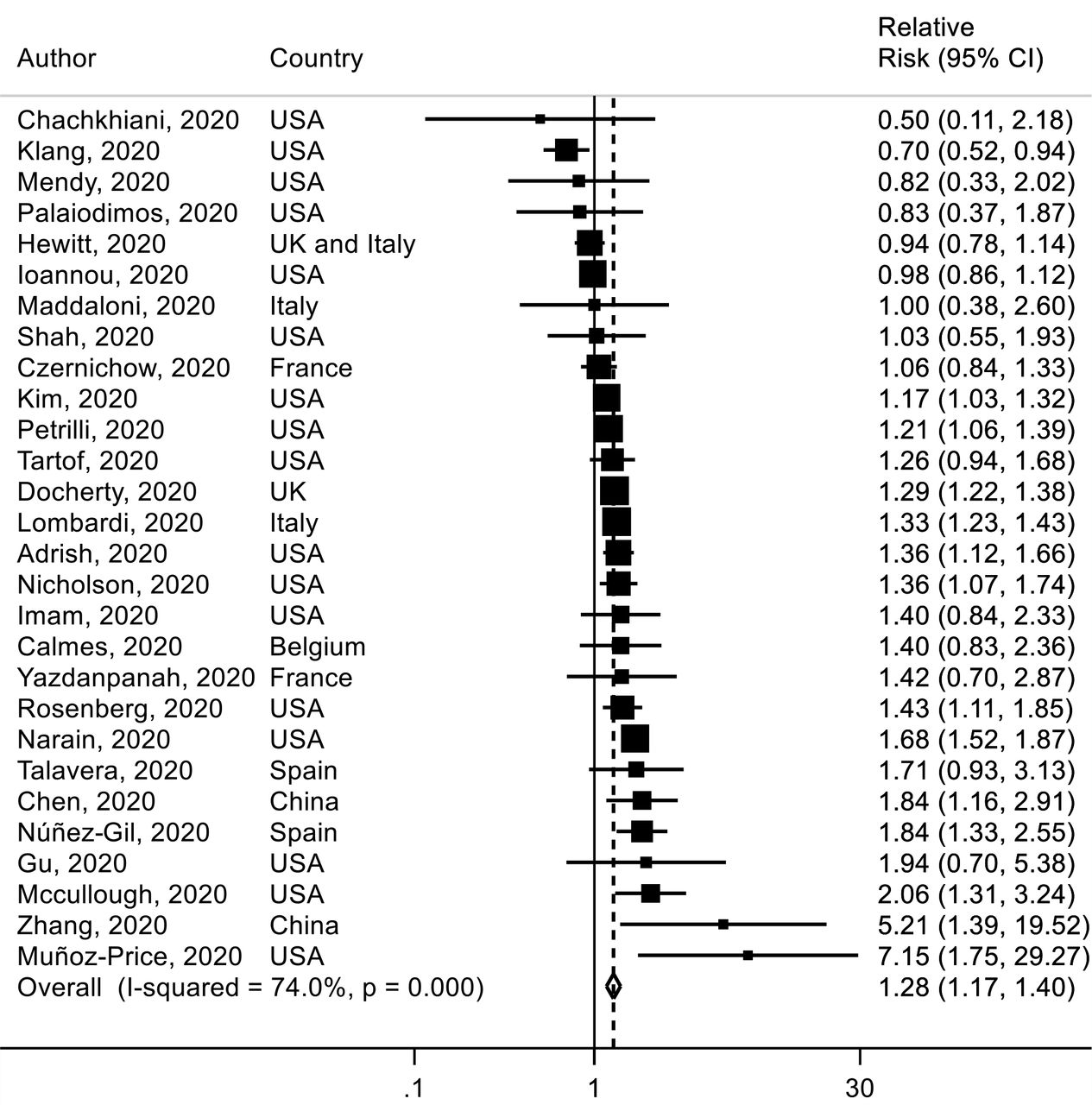
Twenty-eight studies38 40 58 61 63 66 67 76 93 97 103 108 110 111 118 121 129 161 164–166 175 177 183 232 236–238 were included in the analysis of ever smoking versus never smoking and mortality with a total of 11 333 deaths among 47 096 patients with COVID-19. The SRR for hospital death in patient with COVID-19 was 1.28 (95% CI 1.17 to 1.40, I2=74%) for ever smokers versus never smokers (figure 5). The absolute risk of death for smoking was increased by 7% (table 1). There was no evidence of publication or small study bias (p value=0.91) (online supplemental figure 9). In sensitivity analyses, the results persisted when excluding one study at a time (online supplemental figure 10).
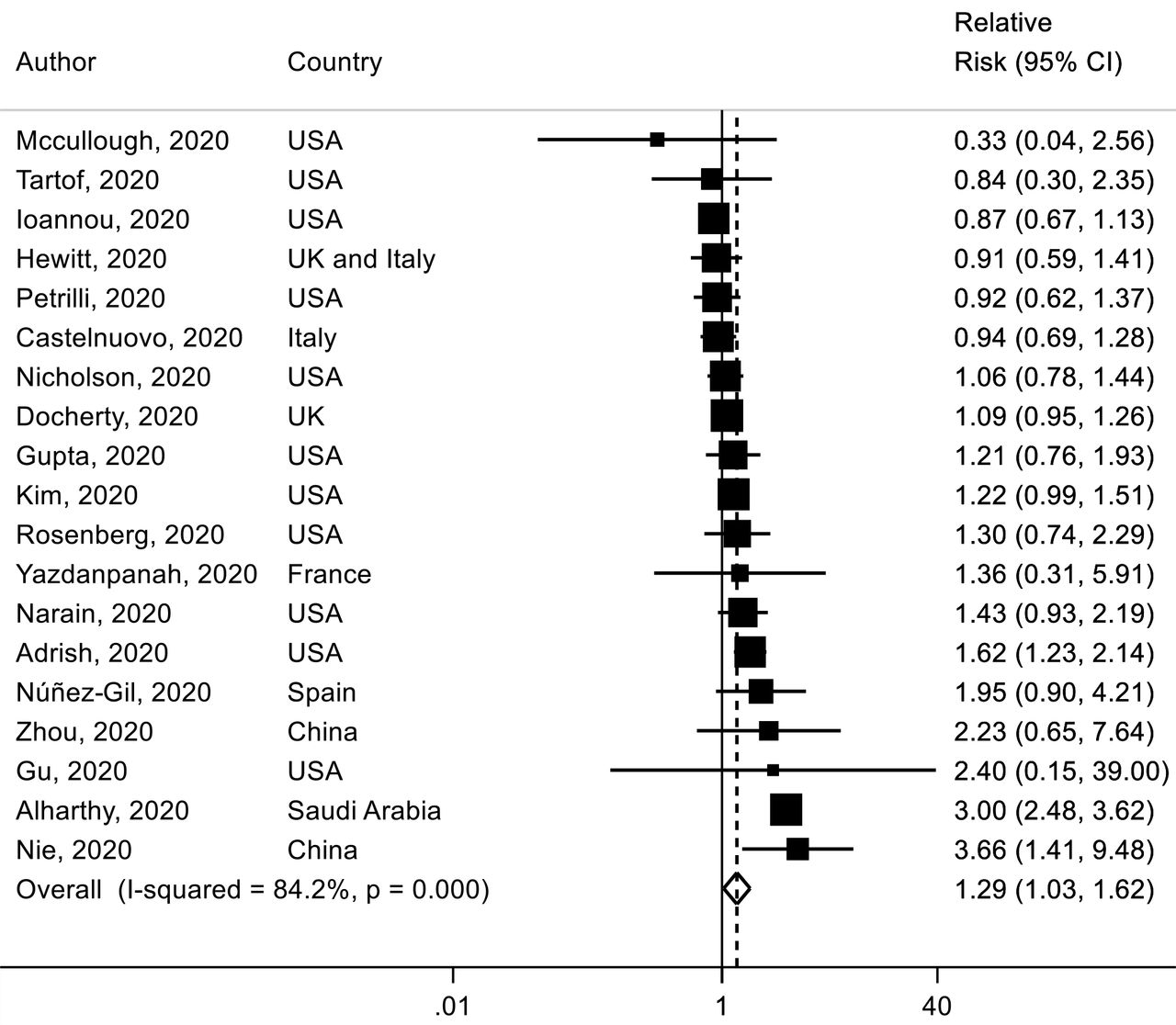
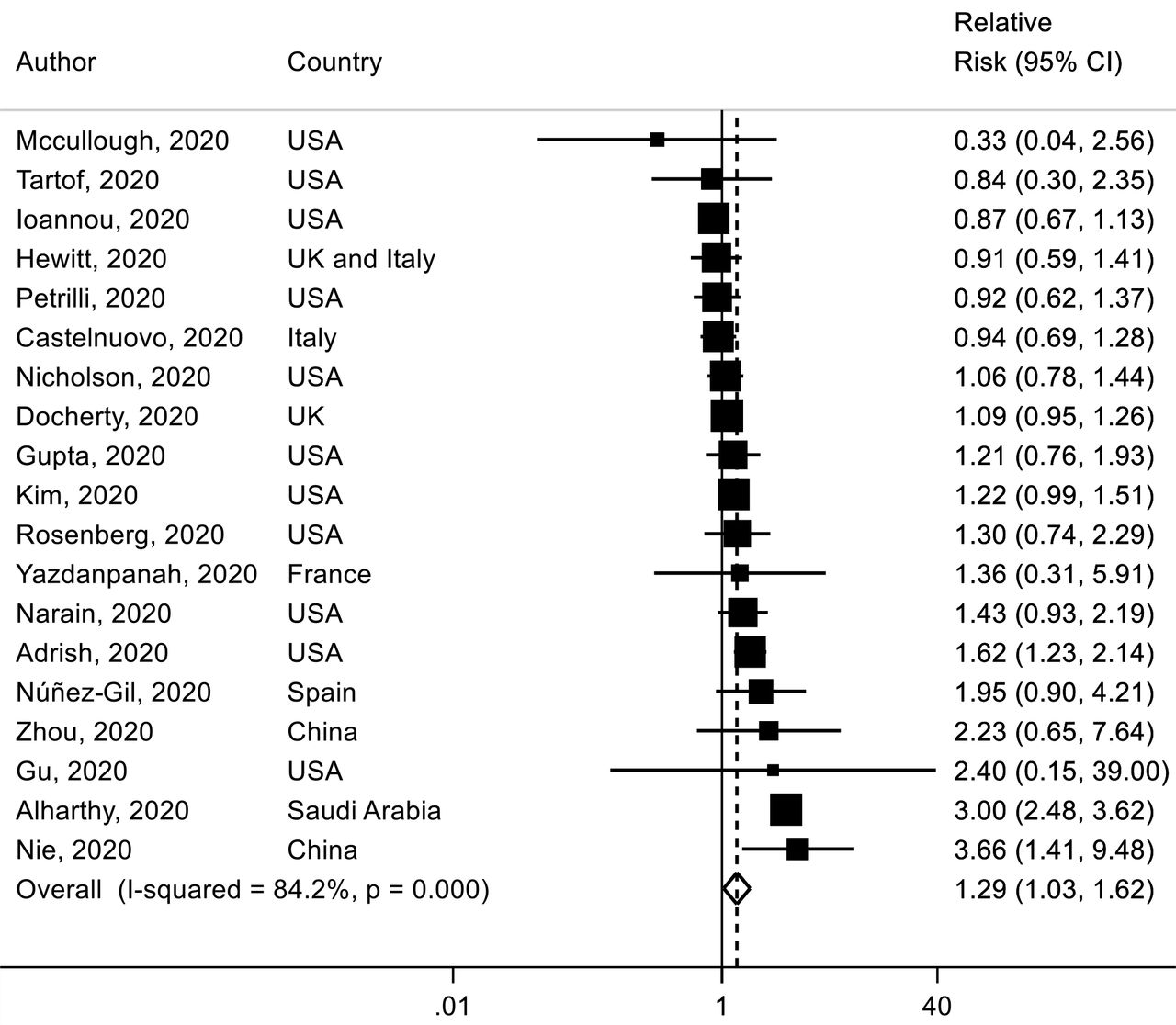
For current smoking versus never smoking, nineteen studies,4 58 66 76 97 103 110 111 117 118 121 129 161 162 165 177 203 236 239 which included 9845 deaths among 33 147 patients with COVID-19, were identified. The SRR of current smoking was 1.29 (95% CI 1.03 to 1.62, I2=84%) (figure 6) and no statistically significant evidence of publication bias was observed (p value=0.86) (online supplemental figure 11).
A total of 14 studies58 66 76 97 103 110 111 118 121 129 161 165 177 236 were included in the analysis of former smoking versus never smoking and mortality risk, including 8121 deaths among 25 340 patients with COVID-19. The SRR was 1.25 (95% CI 1.11 to 1.42) with moderate to high heterogeneity (I2=75%) (figure 7). There was no evidence of publication bias with Egger’s test (p value=0.70). In sensitivity analyses excluding one study at a time from the analyses of current and former smoking, the results were not materially altered (online supplemental figures 12-13). Globally, results did not change in nearly all subgroup analyses (online supplemental table 4).
Finally, a total of 15 studies29 44 52 58 107 174 186 192 208 218 240–243 did not provide a definition of the smoking variable (>76 400 deaths, 682 310 patients) and the SRR was 1.31 (95% CI 1.07 to 1.62, I2=88%) (online supplemental figure 14) which seemed to be similar to current and ever smoking.
PAF of deaths and assessment of certainty of the body of evidence
The estimated PAF was 10.6%, 11.8%, 11.5% and 2.5% for diabetes, hypertension, obesity and ever smoking, respectively when considering all studies included in this meta-analysis (table 1). Based on studies that adjusted for multiple risk factors, attributable death was 8% for diabetes, 7% for hypertension, 11% for obesity and 2% for ever smoking.
Regarding the body of evidence, certainty of evidence was rated ‘low’ for diabetes, hypertension and smoking and ‘high’ for obesity (online supplemental table 5).
Discussion
Principal findings
To our knowledge, this study is one of the largest meta-analyses of association between diabetes, hypertension, obesity, smoking and COVID-19 mortality. We found that patients with diabetes had a 54% higher risk of death from COVID-19 compared with patients without diabetes; those with hypertension had a 42% increase in the relative risk of death from COVID-19 compared with patients without hypertension and those with obesity have a 45% greater in the relative risk of COVID-19 death compared with non-obese patients. In addition, we found that ever, current and former smoking was associated with 28%, 29% and 25% increases in the relative risk of death in patients with COVID-19. Our linear dose–response meta-analysis suggested that each 5 kg/km2 increment in BMI was associated with a 12% greater risk of COVID-19 death. However, evidence of non-linearity was observed in the analysis of BMI and risk of COVID-19 death, with a J-shaped dose–response relation with flattening of the dose–response curve between 22 and 24 of BMI level and a slight increase below that range and a 1.5–2-fold increase in risk with a BMI of 40–45. While there was no publication bias, study heterogeneity was high for all exposure and this persisted in most of the subgroup analyses. However, the heterogeneity appeared to be driven to a larger extent by differences in the strength of the associations, than differences in the direction of the effect, as the vast majority of studies reported significant or non-significant positive associations between these exposures and increased mortality, and relatively few studies reported risk estimates in the direction of an inverse association. Given this meta-analysis included more studies than a typical meta-analysis, I2 and heterogeneity were high as the likelihood of divergent findings increases with increasing number of studies.
Comparisons to findings from previous epidemiological studies and biological mechanisms
Since the first reports of COVID-19, several studies have shown that patients with COVID-19 with comorbidities have a higher risk of death.4 17 244 245 However, these studies have differed greatly in term of sample size, and results are conflicting and heterogeneous. Previous meta-analyses have shown that patients with diabetes, hypertension and obesity had an increased risk of mortality.16–18 21 246 247 Unfortunately, these previous meta-analyses were limited by the lack of subgroup analyses, which is crucial to evaluate heterogeneity and no previous meta-analysis has estimated the number of deaths attributed to these comorbidities or conditions.
This meta-analysis summarises the results of 186 observational studies published up to November 2020, including 210 447 deaths among 1 304 587 million patients with COVID-19. Our findings are similar to results from previously published systematic reviews, suggesting a higher mortality rate of COVID-19 in patients with cardiovascular or chronic condition.16 17 21 22 We found a 1.54-fold greater mortality from COVID-19 among patient with diabetes compared with those without (n=145 studies), which is similar to those yielded in previous meta-analyses,16 whereas the estimate magnitude is weaker than those in de Almeida-Pititto et al,21 Kumar et al,246 Shang et al248 and Luo et al.17 In our subgroup analyses, we found that the positive association was stronger in studies without any adjustment or adjusted for age only compared with studies that adjusted for multiple factors. Thus, the higher magnitude observed in the previous meta-analyses may be in part due to the important number of studies without adjustment for confounding factors such as age and comorbidities, which are mostly with critical or serious risk of bias. In addition, we estimated that 8% of deaths by COVID-19 were attributed to diabetes; this aspect has to our knowledge not been investigated previously. The absolute risk of death associated with diabetes was increased by 14%. The mechanism underlying the increased mortality from COVID-19 in patients with diabetes may be explained by chronic inflammatory conditions. Patients with COVID-19 with diabetes have a significantly higher inflammatory markers such as C reactive protein (CRP), interleukin 6 (IL-6) compared with patients without diabetes.249 Inflammatory markers such as IL-6, CRP, IL-10, lactate dehydrogenase and tumor necrosis factor-α, which are indicative of different aspects of COVID-19 severity, requirements of intensive care support including dialysis and ventilation, are associated with higher risk of death.250 251
Regarding hypertension, our findings yielded a 1.42-fold higher risk of death from COVID-19 in patient with hypertension (n=127 studies), which also is slightly weaker than the results from previous meta-analyses.16 22 247 Nearly 7% of death in patients with COVID-19 could be attributed to hypertension and we found that hypertension increased the absolute risk of death by 11%. Previous clinical studies showed that hypertension is a major risk factor for worse outcome in patients infected with SARS and Middle East respiratory syndrome.252 253 Although, the exact mechanism by which hypertension increase mortality rate remains unclear, chronic inflammation may play an active role in increasing risk of death.
Du et al suggested that patients with obesity had a 2.68-fold risk for COVID-19 mortality compared with non-obese patients (n=7 studies).18 In dose–response analysis, they showed that for each 1 kg/m2 increase in BMI, the risk of death increased by 6%. Partly consistent with this study, we found that a 5 kg/m2 increase in BMI level was associated with a 12% increase in the risk of death in patient with COVID-19 (n=25 studies). In addition, we found evidence of a non-linear J-shaped association between BMI and mortality from COVID-19, with a flattening of the dose–response curve for BMI values between 22 and 24 kg/m2 and with a slightly higher risk below that range and a moderate to strong increase in mortality with severe obesity (BMI 40–45). Obesity is associated with a low-grade systemic inflammation, which plays a major role in the pathogenesis of respiratory conditions. Patients with COVID-19 and with preexisting obesity may have an overactivated inflammation response, which may induce excessive inflammatory response.254 Obesity is also strongly associated with increased risk of diabetes, hypertension and several other chronic diseases255 that increases risk of COVID-19 mortality.256
In addition, our finding showed that ever, current and former smoking was associated with 28%, 29% and 25% increases in the relative risk of death in patients with COVID-19 compared with never smokers. Tobacco smoking is known to alter the function of the immune system; therefore smokers are more likely to get a severe infection of COVID-19 due to their poor mucociliary clearance, which could lead to the release of pro-inflammatory markers and oxidative stress and thereby contribute to higher mortality rates. The risk of death in former smokers was higher than in never smokers and only slightly lower than risk in current smoker. However, more studies are required to clarify the impact of longer durations of smoking cessation in former smokers on risk of death in patients with COVID-19.
Although we found that diabetes, hypertension, BMI and smoking were associated with greater COVID-19 mortality, a recent meta-analysis suggested that mortality was more frequently observed in patients with COVID-19 with cardiovascular disease, cerebrovascular accident and chronic kidney disease.257 The authors observed that COVID-19 mortality among all comorbidities was high in European and Latin American patients compared with the US patients. It is possible that geographical differences in therapeutic practice of COVID-19 such as the use of antibiotics, antivirals and others drugs may partly explain the greater COVID-19 death in some regions,258 while there was no evidence of heterogeneity in findings across geographic location in our study. The review also suggested that COVID-19 mortality among those with underlying medical diseases was high in mostly elderly patients.258 However, we did not perform subgroup analysis by age because this information was lacking in most of the included studies.
Strengths, limitations and public health implications
This present meta-analysis of observational studies on diabetes, hypertension, obesity and smoking and risk of death in patients with COVID-19 has several strengths, including the large sample size and number of COVID-19 deaths, the detailed subgroup and sensitivity analyses, as well as the linear and non-linear dose–response analyses, which clarified the strength and shape of the dose–response relationship. Original aspects of our study included the estimation of the number of deaths attributable to these conditions. This is, to our knowledge, the first meta-analysis that perform a separate analysis of ever, current and former smoking versus never smoking in relation to COVID-19 mortality. As any previous published meta-analyses, the current analysis has some limitations that should be considered in the interpretation of our findings. First, we did not investigate the association between presence of two or more coexisting comorbidities and risk of death in patients with COVID-19. Finally, subgroup analyses stratified by clinical or lifestyle factors such as medications, diabetes type and duration, adherence to specific diet, or physical activity were not possible because of the lack of such data from the studies included.
Despite these limitations, our findings may have important public health implications in the context of increasing numbers of severe COVID-19 cases, overburdened hospitals and leading to higher hospital death due to COVID-19 and suggest that people with cardiovascular risk factors, in particular those with diabetes, hypertension and obesity, should be considered as a high priority to get vaccinated. In addition, since smoking is a risk factor for several chronic diseases, including cancer and cardiovascular disease, our finding lend support to the importance of smoking prevention and smoking cessation and support policies and public health efforts to reduce the prevalence smoking in the general population.
Conclusion
Our finding suggests that presence of diabetes, hypertension, obesity and smoking in patients with COVID-19 is associated with a 1.54-fold, 1.42-fold, 1.45-fold and 1.28-fold greater risk of mortality, respectively. We have found that the proportion of death attributable to diabetes, hypertension, obesity and smoking was 8%, 7%, 11% and 2%, respectively. These findings support that people with diabetes, hypertension, obesity should be prioritised for vaccination in order to limit the higher death rates in hospital. Public policies should promote a healthier lifestyle including healthier diets and regular physical activity to reduce patient risk factors and comorbidities.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
DA and GS are joint senior authors.
Twitter @MS_Yahya_, @T_Fiolet, @Damkyan_Omega, @AnthonyGuihur
Contributors YM-S conceived and designed the research. YM-S performed statistical analysis and wrote the first draft of the paper. YM-S, TF and MER performed the literature search and literature screening. YM-S and TF assessed the risk of bias of the studies and assessed the certainty of evidence of the associations. MM assisted with the statistical analysis. YM-S, TF, MER, MM, AG, DEF, NL, NP-S, DA and GS contributed to data interpretation and revision of the manuscript for intellectual content. YM-S takes responsibility for the integrity of the data and the accuracy of the data analysis. YM-S is responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.