Article Text

Abstract
Objectives: Cardiac autonomic neuropathy (CAN) as a result of diabetic autonomic neuropathy is positively related to a poor prognosis in diabetic patients. The measurement of heart rate variability (HRV) is a remarkable index of cardiac autonomic dysfunction. The aim of this study was to examine the effects of long-term exercise training on HRV in type 2 diabetic patients with definite CAN.
Methods: Seventeen type 2 diabetic patients with definite CAN (group A: 56.2 years (SD 5.8)) and 15 without CAN (group B: 55.8 years (SD 5.6)) participated in the study. All patients followed an aerobic exercise training programme three times a week for 6 months; the intensity of the session was 70% to 85% of heart rate reserve. At the beginning and end of the study all subjects underwent graded maximal exercise testing with spiroergometry for the evaluation of their aerobic capacity (VO2peak). Moreover, time and frequency domain indices of HRV were obtained from 24 h ambulatory continuous ECG Holter recordings.
Results: At baseline, all measurements of HRV indices were significantly reduced in group A compared with group B (p<0.05). Moreover, group A reached a significantly lower VO2peak by 14.8% compared with group B (p<0.05). Following the exercise training programme, the SD of all normal-to-normal RR intervals in the entire recording (SDNN) was increased by 18.8% (p<0.05) and 13.8% (p<0.05), the square root of the average of sum of squares of difference between adjacent filtered RR intervals (rMSSd) was increased by 35% (p<0.05) and 15.2% (p<0.05), and the percentage of differences between adjacent filtered RR intervals which was greater than 50 ms for the entire analysis (pNN50) was increased by 400% (p<0.05) and 67.9% (p<0.05) in groups A and B, respectively. Regarding the frequency domain indices, only the high frequency power (HF) was found to be significantly increased in group A. At the end of the exercise training programme, SDNN, rMSSd and low frequency power (LF) were significantly lower (24.3% (p<0.05), 20.3% (p<0.05) and 40% (p<0.05), respectively) in group A compared with group B. Also, VO2peak increased by 17.8% (p<0.05) in group A and by 11% (p<0.05) in group B. Furthermore, the exercise training programme had significant effects on blood lipid and glucose levels and glycosylated haemoglobin (HbA1c) in both groups.
Conclusions: The results indicate that 6-month aerobic exercise training improves the cardiac autonomic nervous system function in type 2 diabetic patients. However, more favourable effects are found in type 2 diabetic patients with definite CAN.
Statistics from Altmetric.com
A very serious and common complication of diabetes mellitus (DM) is diabetic autonomic neuropathy (DAN), which can occur as early as the first year after diagnosis of DM and may lead to cardiovascular, gastrointestinal and genitourinary system dysfunction. Manifestations of DAN affecting these systems greatly contribute to increased morbidity and mortality, as well as reduced quality of life among patients with diabetes.1 Cardiac autonomic neuropathy (CAN) is the most clinically important and well-studied form of DAN, due to its association with a wide spectrum of adverse cardiovascular outcomes.2 The prevalence rate of borderline or definite CAN is 8.5% to 16.8% among type 1 diabetic patients and 12.2% to 22.1% among type 2 diabetic patients, respectively.3 Several epidemiological studies have shown that the 5-year mortality rate is five times higher in patients with DM and CAN, as compared to those without CAN.4 The causes of death among diabetic patients with CAN are quite variable, including myocardial infarction, congestive heart failure, neuropathic cardiomyopathy, malignant ventricular arrhythmias, progressive renal failure and respiratory problems due to impaired hypoxia-induced respiratory drive.5–7
Abnormalities in cardiac autonomic function manifested by abnormal heart rate and blood pressure responses to exercise were mainly noticed in DM patients with CAN.8 The severity of CAN was also found to be inversely correlated to achieved heart rate during submaximal or maximal effort.9 Moreover, a decreased cardiac output adjustment to exercise was observed in diabetic patients with CAN.10 The cardiorespiratory performance of diabetic patients is found to be limited in comparison with aged-matched healthy sedentary individuals.11 Furthermore, the work capacity of diabetic patients with CAN has been proved to be more reduced than that of diabetic patients without CAN, mainly due to the abnormal cardiac autonomic modulation.8–10
Heart rate variability (HRV) measurement is an important predictor of cardiac autonomic function.12 It was demonstrated that HRV time and frequency domain indices were depressed in chronic diseases, and were associated with cardiac autonomic dysfunction.13 Systematic exercise training has been shown to improve HRV indices in chronic disease patients with autonomic dysfunction. Thus, in patients with end-stage renal disease on hemodialysis13 and chronic congestive heart failure,14–16 as well those who had undergone coronary angioplasty17 18 and with recent myocardial infarction,19–21 systematic endurance training was shown to trigger improvement, mainly in the parasympathetic outflow, and reduce the incidence of cardiac arrhythmias. In type 2 DM patients with early involvement of CAN, a 12-week moderate-intensity aerobic exercise programme was found to improve HRV indices.22 However, this kind of training produced no change in patients with definite or severe CAN. Moreover, a 12-month exercise programme improved baroreflex sensitivity in patients with type 2 diabetes, but had no beneficial effects on HRV indices.23
The hypothesis of this study was that a training programme with higher workload and increased duration would improve the HRV of patients with definite CAN. Therefore, we investigated the effects of long-term moderate-to-high-intensity aerobic training on cardiac autonomic function in type 2 diabetic patients with definite CAN.
METHODS
Patient selection
Two hundred patients with DM type 2 referred from the diabetes outpatient clinic of the General Hospital Papageorgiou were screened for definite CAN using four noninvasive methods: (1) Valsalva manoeuvre, (2) beat-to-beat variability during periods of inspiration–expiration, and (3) heart rate and (4) blood pressure responses to standing. Heart rate was measured using a 12-lead electrocardiogram and blood pressure with a mercurial sphygmomanometer. The cut-off value of the heart rate responses during the Valsalva manoeuvre was 1.10, beat-to-beat variability of inspiration–expiration was 10.00, and beat-to-beat variability from sitting to standing was 1.00.24 Additionally, the cut-off value of the blood pressure response from sitting to standing was 30 mm Hg.24 According to Ewing et al (1985)24 early involvement of CAN was established if one of the three heart rate tests was abnormal or two were borderline, definite involvement of CAN was recognized in cases where two or more of the heart rate tests were abnormal and severe involvement of CAN was acknowledged where two or more of the heart rate tests and the blood pressure test were abnormal. In our study, 30 patients were diagnosed with definite CAN and 170 without CAN.
The following exclusion criteria from the study were employed: clinical evidence of coronary artery disease or heart failure, chronic obstructive pulmonary disease, proliferative diabetic retinopathy (including patients who underwent laser treatment), and any kind of neurological or orthopaedic problem that would render the patient unable to follow the exercise training programme. Nineteen patients with definite CAN were selected (group A: 8 men and 11 women) who were free from other chronic diseases. Out of the initial sample, 70 patients without CAN were found to have no evidence of other chronic diseases. From this pool 19 patients without CAN were randomly chosen by lottery (group B: 5 men and 14 women). The number of patients using antihypertensive (diuretics or AT-receptor or calcium channel blocker) and cholesterol-lowering medications was almost the same in both groups. All patients were receiving oral hypoglycaemic agents for the treatment of diabetes: 12 patients were treated with metformin, 7 patients with sulfonylureas and 19 with a combination of the two. No patient was taking beta-blockers, ACE inhibitors or other antiarrhythmic drugs.
All patients were informed about the purpose and the procedures of the study and signed an informed consent form, according to the Code of Medical Ethics of the Research Committee of the Aristotle University of Thessaloniki. None of the patients had participated in any form of regular exercise during the past year. They were asked to refrain from any other form of recreational activity during the study period. The medication regimen of the participating patients was not altered throughout the duration of the study.
Study design
At the beginning and end of the 6-month study period, all patients underwent a physical examination, blood analysis, electrocardiogram, 24 h Holter ambulatory ECG monitoring and exercise stress testing in combination with spiroergometry. The test procedures were executed in the morning from 09:00 to 11:00. All patients were advised not to participate in any kind of physical activity for 48 h before their examination and to refrain from smoking and consuming any kind of food, coffee and carbohydrates or electrolytes for 3 h before their examination. Medication other than oral hypoglycaemic agents was discontinued 48 h before testing. The investigators for the blood analysis, spiroergometry and Holter analysis were blinded regarding the condition and treatment of the patients.
Blood analysis
Following a 10–12 h overnight fast, blood was drawn via an antecubital vein for analysis. All blood measurements were taken at least 1 week before training began and 48 h after the last training session. The biochemical examinations included detection of glucose, cholesterol, triglyceride, high-density lipoprotein (HDL) and low-density lipoprotein (LDL) levels and were conducted using an Olympus AU 400-type analyser (Olympus Diagnostica, GmbH, O'Callaghan's Mills, Ireland). Glycosylated haemoglobin (HbA1c) was assessed by the monoclonal antibody method using a DSA 2000-type (Bayer, Russelsheim, Germany) analyser.
Spiroergometry
The symptom-limited exercise test was performed on a motor-driven treadmill according to a multistage Naughton protocol. Patients were encouraged to exercise until subjective exhaustion. Exercise was considered maximal if a plateau in O2 consumption was obtained despite an increase in effort, or if the presence of a respiratory exchange ratio (VCO2/VO2) was greater than 1.00 and if age-predicted maximal heart rate was attained. Blood pressure was measured at the end of each 3 min stage, while the electrocardiogram monitoring was continuous (CH-2000, Cambridge Heart Co., Bedford, Massachusetts, USA). To assess aerobic exercise capacity, peak oxygen consumption (VO2peak) was measured by breath-by-breath gas analysis using a spiroergometer device (Quark b2, Vesion 6.0, Cosmed, Rome, Italy), which was calibrated according to the specifications of the manufacturer before each test began. The Quark b2 system is equipped with fast analysers for O2 and CO2 with response times of <120 ms and <150 ms, respectively. This allows the spiroergometer system to get accurate results, even when a high respiratory frequency is achieved. VO2peak was defined as the highest VO2 attained during the exercise test. Maximal pulmonary ventilation (Vemax) and tidal volume (VTmax) were also assessed.
Holter monitoring
Twenty-four-hour ambulatory ECG monitoring was obtained in all patients using a 3-channel ECG digital Holter recorder (GBI-3S, Galix Biomedical Instrumentation, Miami, Florida, USA). Patients were asked to perform only their usual daily activities during monitoring. The electrocardiographic recordings were digitized at 500 samples per second. The data were stored in a standard PCMCIA memory card and then analysed by a specially designed software program. A blinded investigator both automatically and manually discarded artifacts, ectopic beats, premature atrial and ventricular complexes and the subsequent interval. The frequency analysis was based on applying the fast Fourier transform (FFT). The RR signal was converted to heart rate, linearly interpolated and graphed in regular intervals of 0.5 seconds (2 Hz). In this way, 288 segments representing 5-minute heart rate signals were obtained and multiplied by a Hanning window.
For the evaluation of HRV, the time domain and frequency domain analyses were used. From time domain analysis, three HRV indices were measured: (1) the SD of all normal-to-normal RR intervals in the entire recording (SDNN); (2) the square root of the average of sum of squares of difference between adjacent filtered RR intervals (rMSSd); and (3) the percentage of differences between adjacent filtered RR intervals which was greater than 50 ms for the entire analysis (pNN50). From frequency domain analysis, two different frequencies were reported in addition to total power: high-frequency power (HF) (0.15–0.4 Hz) and low-frequency power (LF) (0.04–0.15 Hz). According to the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology, the pNN50, rMSSd and HF domain represent vagally mediated respiratory variations, whereas the LF domain is mediated both sympathetically and parasympathetically.5 Moreover, LF and HF were estimated in normalized units and the LF to HF ratio was calculated as a measure of autonomic balance.
Exercise training programme
The exercise intervention was structured and supervised by a group of experienced rehabilitation exercise trainers in a public gym. The 6-month training regimen consisted of three sessions of aerobic exercises per week. During the training sessions heart rate was continuously monitored by specific telemetric devices (Polar, Heart Rate Monitors, New York, USA), while blood pressure was measured in each interval by a mercurial sphygmomanometer. The intensity of each exercise session was 70% to 85% of the heart rate reserve (HRR).25 The duration of the exercise session was initially 45 min and reached 75 min after the first 3 months. Each session commenced and concluded with a 10–15-minute warm-up/cool-down period, which included cycling, stretching exercises and breathing exercise drills. The main training programme involved interval aerobic exercises, which included calisthenics and steps.
Statistical analysis
Statistical analyses were performed using the SPSS 12.0 for Windows (Statistical Package for Social Sciences, Chicago, IL, USA). Data are expressed as the mean (SD). For comparison among groups, two-way analysis of variance (ANOVA) with repeated measures of both factors (group*time), followed by simple main effect analysis was conducted. In order to determine the relationship between HRV and cardiorespiratory indices, correlation coefficients, according to Spearman, were calculated. Additionally, the relationships of the differences from the final to the initial measurement of the above parameters were calculated. A p value of <0.05 was considered as statistically significant.
RESULTS
Two patients from group A and four from group B of the original 38 patients who took part in the training programme were excluded from the final analysis. One group A patient had lumbar spine problems and the other was unable to fulfill the 70% attendance required during the training programme. In group B, one patient was diagnosed with breast cancer, one had a stroke event and two were unable to fulfill the 70% attendance requirement. The demographic and clinical characteristics of the 32 patients with type 2 diabetes that completed the exercise training programme are shown in table 1 (and table 2).
Pretraining data
The blood analysis results are listed in table 3. There was no statistically significant difference between the two groups regarding glucose and HbA1c. On the other hand, cholesterol and HDL were found to be reduced in group A by 8.3% (p<0.05) and 26% (p<0.05), respectively, as compared to group B, and LDL was decreased by 9.2% (p<0.05) in group A as compared to group B.
At maximal exercise test on the treadmill, group A reached lower VO2peak by 14.8% (p<0.05) and Vemax by 18.3% (p = 0.07) as compared to group B (table 4). However, no significant differences were found between the two groups with respect to test duration, peak heart rate, and systolic and diastolic blood pressure.
Table 5 shows the data from both time and frequency domain HRV analysis. In the time domain analysis significant differences were found in all variables between the two groups. During the 24 h Holter monitoring 59% of the patients in group A and 53% in group B had arrhythmias (Lown class II or higher), such as atrial or ventricular extrasystoles, multiform extrasystoles and transient tachycardias. The SDNN, rMSSd and pNN50 were found to be significantly reduced by 26% (p<0.05), 27% (p<0.05) and 63% (p<0.05), respectively, in group A as compared to group B. In the frequency domain analysis the LF and HF were significantly lower in group A by 50% (p<0.05) and 47.7% (p<0.05), respectively; there was no significant difference between the two groups regarding the LF:HF ratio.
During the baseline measurements, a positive linear relationship was observed only in group A between the LF:HF ratio and the test duration (r = 0.650, p<0.05).
Post-training data
The exercise training programme had favourable effects on blood lipid and glucose levels and HbA1c in both groups (table 3). In groups A and B the glucose level was decreased by 19% (p<0.05) and 10.6% (p<0.05), respectively. Additionally, HDL was considerably increased in group A by 23.9% (p = 0.02) and in group B by 9.4% (p = 0.05), while LDL was significantly decreased by 13.7% (p<0.05) in group B. Also, HbA1c was significantly decreased in group A by 10% (p<0.05) and in group B by 9.2% (p<0.05). Cholesterol and HDL were found to be reduced in group A by 10.3% (p<0.05) and 16.2% (p<0.05), respectively, as compared to group B. There was no statistically significant difference between the two groups regarding the final values of glucose, LDL and HbA1c.
At the end of the exercise training programme VO2peak (table 4) increased in group A by 17.8% (p<0.05) and in B by 11% (p<0.05). However, no statistically significant difference was found between the two groups. The Vemax was increased in group B only by 14.5% (p<0.05). Moreover, the average test duration during the treadmill test was significantly increased in group A by 9.2% (p<0.05) and in group B by 9.3% (p<0.05). The resting heart rate was reduced in group A by 12.8% (p<0.05) and in B by 8% (p<0.05). However, the heart rate peak was increased by 6% (p<0.05) in group B only. No difference was observed between the groups regarding peak heart rate.
As compared to baseline data fewer patients in group A (47%) and in group B (49%) had arrhythmias. The analysis of HRV parameters revealed that time domain indices were significantly increased in both groups (table 5). The SDNN was increased by 18.8% (p<0.05) and by 13.8% (p<0.05) in groups A and B, respectively. Moreover, rMSSd and pNN50 were significantly greater by 35% (p<0.05) and by 400% (p<0.05), respectively, in group A, and by 15.2% (p<0.05) and by 67.9% (p<0.05) in group B as compared to baseline values. Spectral power in the HF band indicated a highly significant rise in group A by 70% (p = 0.001) and a borderline amplification in group B by 26.3% (p = 0.07). In the LF band a significant increase by 47.5% (p = 0.01) was observed in group A only. A considerable improvement of the autonomic balance by 14.8% (p<0.05), which is represented by the LF:HF ratio, was observed in group B only. The SDNN and rMSSd were found to be significantly lower by 24.3% (p<0.05) and by 20.3% (p<0.05), respectively, in group A as compared to group B. In the frequency domain analysis the LF was significantly lower in group A by 40% (p<0.05) as compared to group B. No statistically significant differences were found between the groups when comparing the differences from the final to the initial measurement of all the HRV analysis indices.
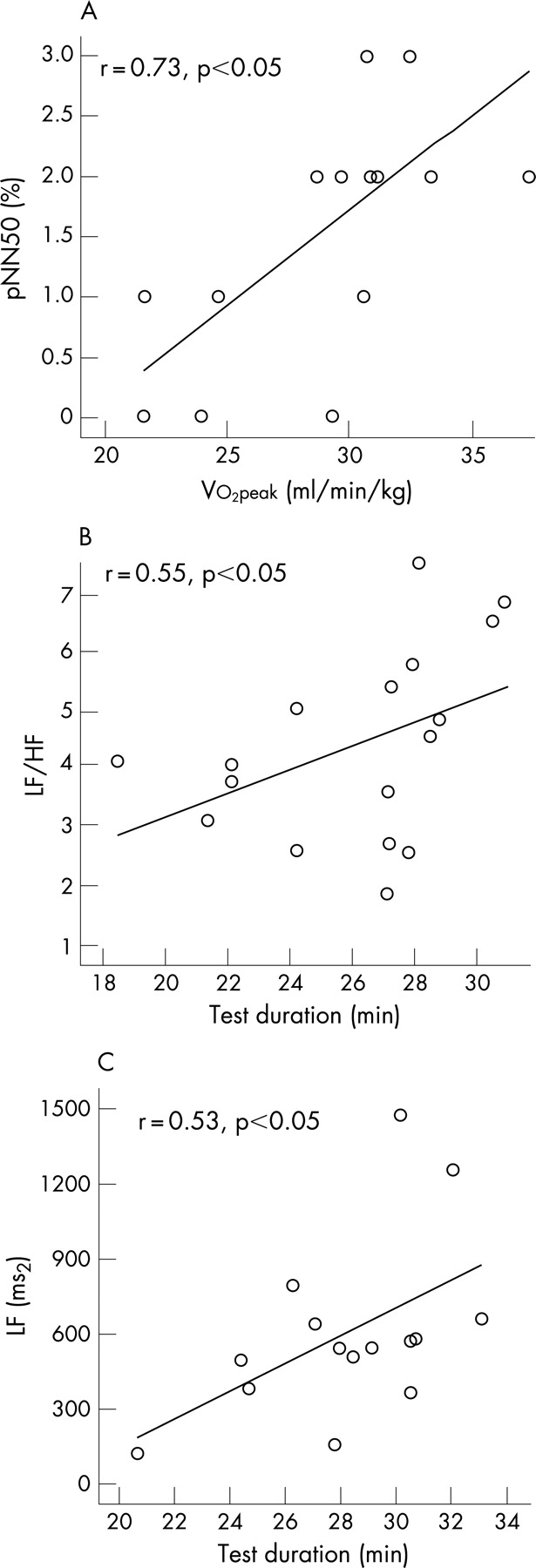
Following the 6-month exercise training programme positive linear relationships were found in group A between pNN50 and VO2peak (r = 0.56, p<0.05, fig 1) and LF:HF and test duration (r = 0.40, p<0.05, fig 1), as well as improvements in pNN50 and HbA1c (ΔpNN50 and ΔHbA1c, r = −0.66, p<0.05, fig 2) and improvements in rMSSd and HbA1c (ΔrMSSd and ΔHbA1c, r = −0.49, p<0.05, fig 2). In group B a positive linear relationship was found only between LF and test duration (r = 0.53, p<0.05, fig 1c).


{kind=link}
{kind=link}
DISCUSSION
Pretraining results indicate that diabetic patients with definite CAN have lower aerobic capacity and impaired HRV as compared to patients without CAN. A 6-month aerobic exercise programme of moderate intensity was capable of improving the cardiac autonomic activity in patients with definite CAN, in addition to increasing aerobic capacity and improving glycemic control and lipidemic profile.
There are several potential reasons for the reduced aerobic capacity observed among diabetic patients with CAN. Τhe restricted cardiac autonomic nervous system activity during exercise, which is necessary for the augmentation of cardiac output and redistribution of blood flow to the working muscle, may limit their ability to perform exercise.8 26 Another possible explanation could be the diminished stroke volume and ejection fraction responses during exercise in diabetic patients with CAN.9 10 Left ventricular diastolic dysfunction commonly seen in diabetic patients is associated with decreased left ventricular compliance and filling, which result in an upward left shift of the left ventricular end-diastolic pressure−volume relation, leading to the limited ability to increase cardiac output by means of the Frank-Starling mechanism during exercise.27 Moreover, insulin deficiency could cause a reduction in aerobic capacity by depleting muscle glycogen stores, which are necessary for the muscles to perform exercise.25 However, in the current study no significant differences were found between the two groups with regard to HbA1c. Therefore, it is unlikely that this mechanism affects the aerobic capacity of our patients with definite CAN. A limited number of studies reported no difference in VO2peak between diabetic patients with and without CAN.28 29 This discrepancy may be attributed to differences in patient selection.
Aerobic training was associated with a significant increase in cardiorespiratory capacity in both groups. It has already been proven that regular physical activity promotes beneficial central and peripheral adaptations in patients with type 2 diabetes mellitus.30–33 The improvement in VO2peak after training in diabetic patients could be due to enhanced oxygen extraction and consumption, increased end-diastolic function and left ventricular mass, and an increase of muscle strength caused by changes in muscle fibre and capillary density in the large body muscles.31 Similar improvements in aerobic capacity, anaerobic threshold and work performance were found in type 2 diabetic patients with or without CAN.22 23 However, there is a discrepancy in the literature regarding the degree of beneficial adaptations, mainly due to differences in the exercise prescription, such as training duration, frequency and intensity of the programme.
According to Vinic et al (2003)34 the duration of the diabetes and poor glycemic control are involved in the development of CAN. Systematic exercise training brings about an improvement in metabolic control, particularly in young and moderately old individuals.30 32 33 Some studies have also found that physical training has beneficial effects on total cholesterol, HDL and LDL levels.31 33 In accordance with these results, our study demonstrated that prolonged aerobic exercise training significantly reduced glucose levels and HDL in both groups.
Our patients with definite CAN showed reduced time and frequency domain indices of HRV as compared to diabetic patients without CAN. This result is in agreement with previous studies.5 34 35 36 According to Schumer et al (1998), CAN is caused by damage to the neural fibres of the autonomic nervous system that normally augment the heart and blood vessels, leading to abnormalities of heart rhythm and vascular dynamics. The natural history of early autonomic involvement is uncertain, although the 5-year mortality rate of diabetic patients with late autonomic neuropathy is high.
The present study demonstrated that 6 months of exercise training caused an improvement in the time and frequency domain HRV indices, indicating an improvement of cardiac parasympathetic and sympathetic activity in both groups. However, the degree of improvement regarding all the parameters measured for the time and frequency domain was greater in group A than in group B. In the literature only a few studies have examined the effects of exercise training on cardiac autonomic activity in diabetic patients with CAN. One study demonstrated that a 12-week training programme in diabetic patients with the early form of CAN led to a significant increase in spectral power of both the LF and HF components.22 This finding supported the theory that exercise training in subjects with early CAN improves both the sympathetic and parasympathetic supply to the cardiovascular system. However, no beneficial effects were found in patients with definite/severe CAN. In contradiction to this, our study demonstrated that 6 months of exercise training improved both spectral and time domain indices of HRV in patients with definite CAN. It is possible that these beneficial effects were the result of a longer period of training in the patients. Moreover, Loimaala et al23 demonstrated that following a 12-month combined endurance and muscle strength training programme, baroreflex sensitivity was improved in patients with type 2 diabetes. Additionally, no significant improvement was observed regarding markers of HRV. In this investigation only asymptomatic patients with type 2 diabetes were studied. In a recent study Zoppini et al (2007)37 showed that a 6-month supervised moderate-endurance training programme improved the sympathovagal balance in patients with type 2 diabetes.
The mechanism by which exercise affects the markers of cardiac autonomic outflow is not clear. There may be a direct involvement of the sinus node because of the bradycardia observed in the resting condition.38 Our study demonstrated that prolonged aerobic exercise training significantly reduced resting heart rate in all diabetic patients. A similar reduction of heart rate was demonstrated by Loimaala et al23 after 12 months of exercise training. Afferent signals from chemoreceptors in the muscles have been shown to control both sympathetic and vagal outflow to the heart through the metaboreflex; thereby autonomic activity is indirectly regulated by the working muscles.39 Furthermore, the exercise-induced alteration of catecholamine concentrations may contribute to the observed autonomic modulation.40 The post-training positive correlation found in our study between pNN50 and VO2peak in group A, and between LF and exercise test duration in group B, could indicate that the improvement in cardiac autonomic function was in part a result of the enhancement of aerobic capacity. Specifically, these results suggest an enhancement of vagal tone by exercise training. Several studies have reported a similar positive correlation between parasympathetic activity and aerobic capacity both in healthy subjects39 40 and in patients with other chronic diseases.13 41 42 However, Loimaala et al23 found that baroreflex sensitivity improvement after exercise training in type 2 diabetic patients correlated significantly with the change in HbA1c, but there was no correlation with changes in VO2peak and central haemodynamics. Similar significant correlations were observed in our patients with definite CAN between the improvement of vagal activity, as indicated by pNN50 and rMSSD, and the improvement of HbA1c. Additionally, studies by Burger et al (1999)43 and Larsen et al (2004)44 showed that fair glycemic control could preserve cardiac autonomic function in patients with type 1 diabetes. Moreover, Manzella et al (2002)45 have demonstrated a negative correlation between B cell function (c-peptide) and sympathetic/parasympathetic balance (LF:HF) in patients with type 2 diabetes.
A potential limitation of the current study is the relatively small number of patients and the absence of untrained diabetic and sedentary health control groups. Moreover, according to the protocol of the study, patients with comorbidity were excluded. The above limitations lead to a restricted generalization of the results. Notwithstanding this limitation it is concluded that aerobic training, as a nonpharmacological intervention, could play a key role in the management of type 2 diabetic patients with definite CAN, mainly by improving cardiac autonomic function and cardiorespiratory performance.
What is already known on this topic
After taking part in a 12-month endurance exercise programme baroreflex sensitivity, but not HRV, was improved in patients with type 2 diabetes without other complications.
In type 2 diabetic patients with early involvement of CAN, a 12-week moderate-intensity aerobic exercise programme was found to improve LF and HF indices of HRV.
What this study adds
A 6-month supervised moderate-endurance exercise training programme improved both frequency and time domain indices of HRV in patients with type 2 diabetes, but, more importantly, exercise training improved parasympathetic autonomic activity in the group of type 2 diabetic patients with definite CAN.
The training programme improved glycemic control and cardiovascular performance in both groups of patients.
REFERENCES
Footnotes
Competing interests: None declared.