Article Text

Abstract
Despite recent progress in identifying and narrowing the gaps in cardiovascular outcomes between men and women, general understanding of how and why cardiovascular disease presentations differ between the sexes remains limited. Sex-specific patterns of cardiac and vascular ageing play an important role and, in fact, begin very early in life. Differences between the sexes in patterns of age-related cardiac remodelling are associated with the relatively greater prevalence in women than in men of heart failure with preserved ejection fraction. Similarly, sex variation in how vascular structure and function change with ageing contributes to differences between men and women in how coronary artery disease manifests typically or atypically over the adult life course. Both hormonal and non-hormonal factors underlie sex differences in cardiovascular ageing and the development of age-related disease. The midlife withdrawal of endogenous oestrogen appears to augment the age-related increase in cardiovascular risk seen in postmenopausal compared with premenopausal women. However, when compared with intrinsic biological differences between men and women that are present throughout life, this menopausal transition may not be as substantial an actor in determining cardiovascular outcomes.
Statistics from Altmetric.com
Introduction
In the decades to come, our society will face greater social, economic and medical challenges due to increasing longevity of the average individual and, in turn, the growing number of older adults in the population at large. The number of persons above age 60 will surpass two billion by the year 2015 worldwide.1 While rapid growth of the older demographic is a well-recognised phenomenon, the health-related heterogeneity of older adults is often under appreciated. Despite the fact that many adults experience increasing morbidity with ageing, many others are able to reach even their 90s in excellent health.2 While almost 10% of adults aged 80 years or older will die within the next 2 years, over half will live on for another decade or more.3 Sex differences are a major contributor to the clinical heterogeneity of older age, especially with respect to cardiovascular disease which is still the leading cause of illness and death in the Western world.
Cardiovascular disease remains essentially an age-related condition in both men and women. Progressive age-related changes in cardiac and vascular anatomy and physiology—collectively referred to as ‘cardiovascular ageing’—interact with cumulative exposure to traditional risk factors to impact an individual's increasing likelihood of developing cardiovascular disease over the life course.4 Much work has been done to understand how these changes predispose to eventual disease at an accelerated rate in some individuals and with more delayed timing in others. Herein, we review the current literature describing sex-specific patterns of cardiac and vascular ageing, and discuss how these patterns likely impact the variations in disease presentations and outcomes that are persistently seen between men and women.
Cardiac ageing
Over the life course, the heart progressively remodels and patterns of cardiac remodeling differ between the sexes (table 1 and figure 1). Typical age-related cardiac remodeling involves increasing left ventricular (LV) wall thickness, decreasing LV dimensions and increasing concentricity, all of which are associated with traditional risk factors and incidence of adverse cardiovascular events.5 ,6 At all ages, men compared with women have greater absolute values of LV mass, wall thickness and cavity dimensions.6 However, with advancing age and adjusting for body size, women experience a more accelerated increase in LV wall thickness than men, especially in the setting of risk factors such as hypertension and diabetes.7 Furthermore, women experience more age-related concentric remodeling than men,8 which may be accompanied by more pronounced diastolic dysfunction.9 With respect to cardiac systolic function, LV ejection fraction (EF) increases with age in both sexes, and this increase is more pronounced in women.10 Women have also been shown to exhibit greater age-related systolic torsion and circumferential shortening of the LV.11 Together, these findings could be due to an augmented pulsatile load in older women12 and differential gene expression of extracellular matrix components in pressure overload states.13 Given that functional oestrogen receptors reside in the myocardium, withdrawal of oestrogens at the time of menopause could also contribute to age-related LV remodeling in women.14
Patterns of cardiac and vascular ageing in men and women
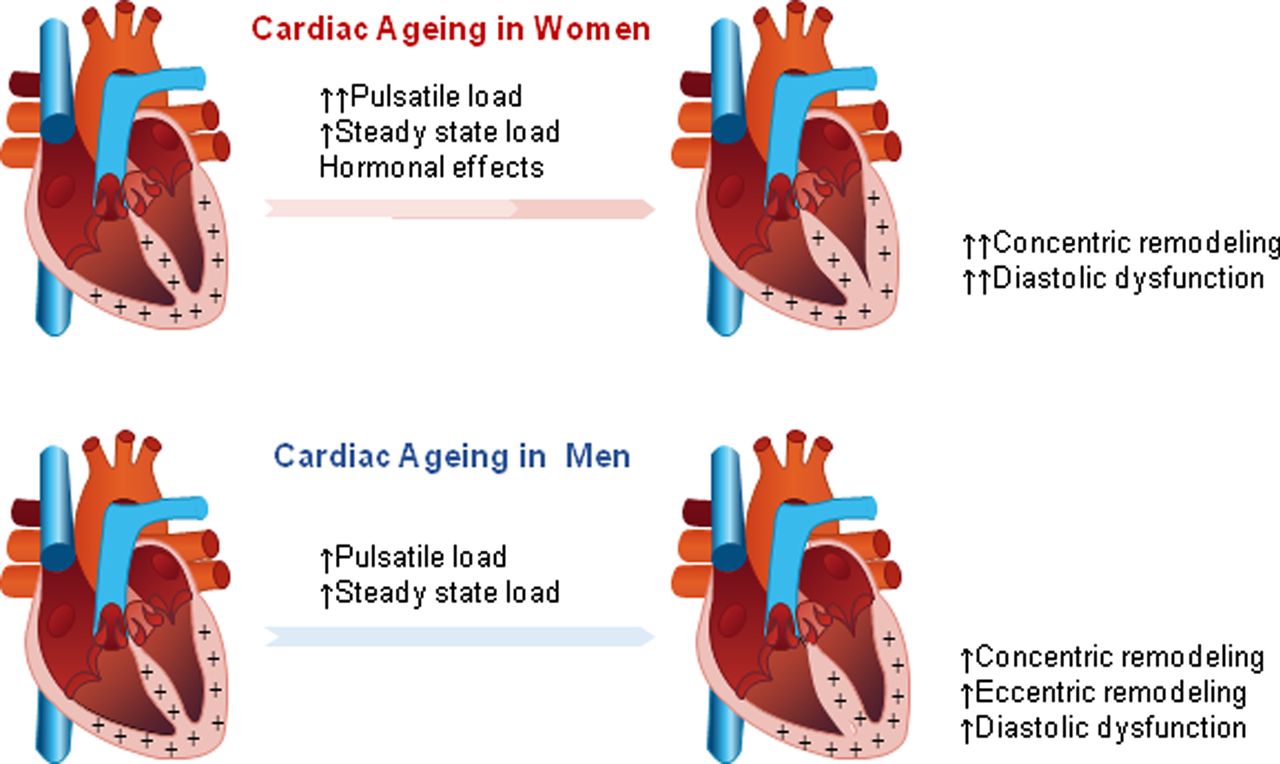
Patterns of cardiac ageing in men and women. ‘+’ symbols represent the presence of oestrogen receptors in the myocardium (including cardiac myocytes and fibroblasts).
Sex differences in cardiac ageing patterns likely contribute to differences in cardiac outcomes (figure 2). Although most data on heart failure (HF) prognosis are derived from randomised trials, wherein women are historically underrepresented, the majority of available evidence suggests that women compared to men with HF have an overall better long-term prognosis.15–17 In particular, the more pronounced concentric remodelling seen in older women than men, along with potentially greater diastolic dysfunction,9 ,18 could contribute to the higher incidence of HF with preserved EF (HFPEF) than reduced EF (HFREF) that is consistently seen more in women than in men.19 In turn, greater rates of HFPEF could account for better HF outcomes seen in women than in men, given that HFPEF is just as likely as HFREF to lead to HF hospitalisations but less likely to lead to HF deaths. Indeed, considerable evidence suggests that the greater prevalence of HFPEF in women contributes to the female survival benefit. Some studies indicate that the female survival benefit for women with HF persists even after adjusting for LVEF and HF aetiology,16 suggesting that sex differences in age-related biology may also contribute to differences in HF outcomes. Accordingly, biomarkers of inflammation (GDF-15, TNF-αR1a), oxidative stress (MPO), remodelling (syndecan, galectin 3), cariomyocyte stretch (NTpro-BNP) and arteriosclerosis (ESAM) have all been shown to have sex-specific prognostic value in HF20; however, the extent to which these findings reflect the greater prevalence of HFPEF in women as opposed to distinct differences between the sexes in HF pathophysiology remains unclear and warrants further investigation.
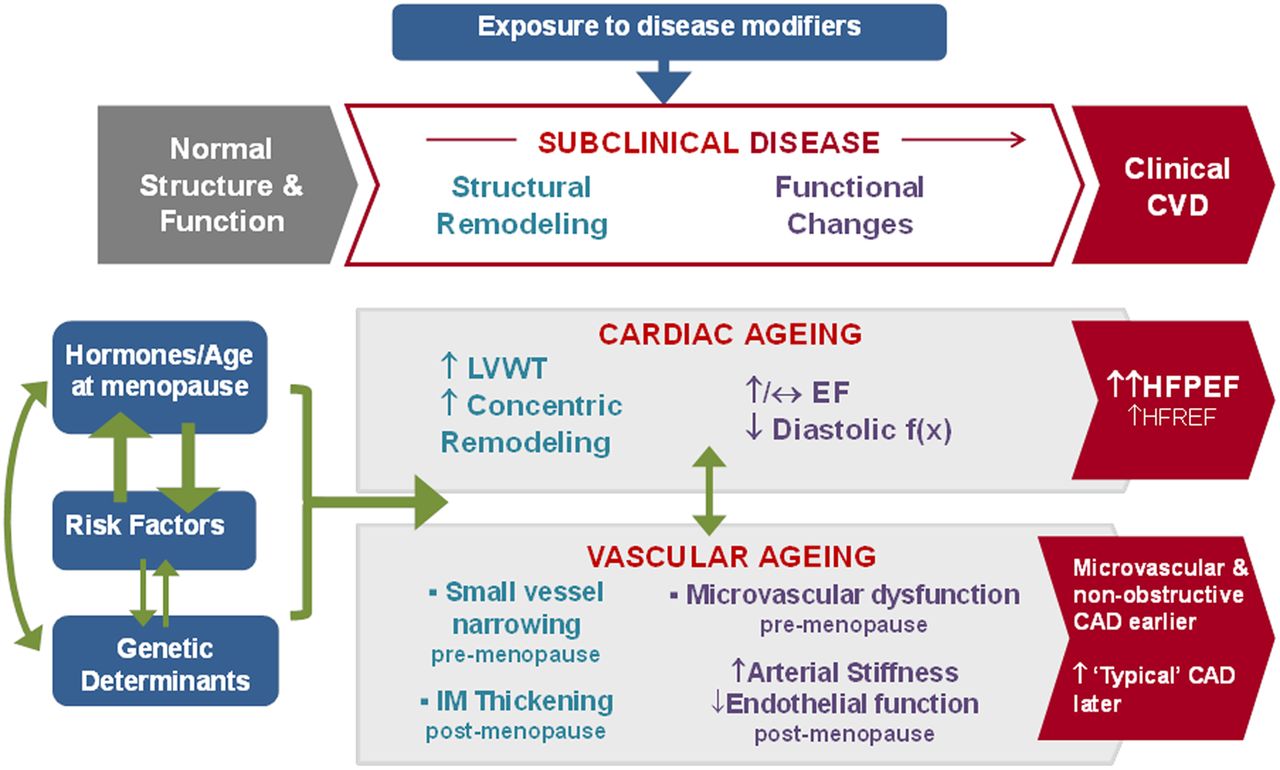
Cardiac and vascular structural and functional ageing processes and the progression to disease in women. Throughout the life course, subclinical changes in cardiac and vascular structure and function interact with traditional pathophysiological disease mechanisms to impact an individual's increasing likelihood of developing disease across the life course. Female-specific disease modifiers and structural and functional changes predispose to different presentations and outcomes compared with men. CAD, coronary artery disease; EF, ejection fraction; HFPEF, heart failure with preserved EF; HFREF, heart failure with reduced EF.
Vascular ageing
As seen with patterns of cardiac ageing, patterns of vascular ageing also differ between the sexes across the life course and these differences have implications for overt disease risk (table 1 and figure 3). Age-related changes in vascular function generally include increasing endothelial dysfunction and arterial stiffness, accompanied by increasing systolic blood pressure and pulse pressure.4 Men have greater endothelial dysfunction and arterial stiffness than women across the age spectrum until the sixth decade, when age-related arterial dysfunction progresses at a faster rate in women. Whereas premenopausal women have lower autonomic tone and baroreceptor response as well as better overall vascular function than men of similar age,21 ,22 postmenopausal women have stiffer arteries than their male counterparts23 even after accounting for body size and aortic diameter.24 These vascular differences are clinically reflected in patterns of hypertension prevalence over the life course: prior to age 45, more men than women have hypertension; between 45 and 64, hypertension rates are similar between the sexes; and at age 65 and above, more women than men are hypertensive (figure 4C).25

Patterns of vascular ageing in men and women. ‘+’ symbols represent the presence of oestrogen receptors in the arterial vasculature (including endothelium, smooth muscle cells and extracellular matrix).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Age-specific death rates attributed to cardiovascular disease and breast cancer and prevalence of hypertension, compiled from US Centers for Disease Control and Prevention data collected from 1999 to 2013. In women, the age-specific death rate due to breast cancer decreases around the time of menopause whereas the age-specific cardiovascular death rate increases steadily across the lifespan (A). In men, cardiovascular death rates decline after midlife whereas continuing to steadily increase across the lifespan in women (B). Prevalence of hypertension is greater in men prior to age 45, similar between the sexes between 45 and 64, and greater in women above age 65 (C). Age-specific death rates for coronary heart disease (D) and heart failure (E).
Subclinical changes in arterial structure also differ between men and women. Carotid intima-media thickening (CIMT), coronary artery calcification (CAC) and carotid and femoral atherosclerotic plaques all increase in prevalence with advancing age.26–28 Although more common in men than in women through midlife, sex differences in the prevalence of subclinical atherosclerosis and coronary calcium are diminished in later life.29 ,30 Nonetheless, men are overall more likely than women to have severe plaques with associated flow disturbance30 as well as high-risk morphologic plaque characteristics31 such as a thin fibrous cap and lipid-rich or necrotic core even after controlling for potential confounders. Interestingly, progression of CIMT is more consistently associated with traditional risk factors in men.32 Because they are highly correlated with traditional risk factors, neither CIMT nor CAC add much prognostic value on top of risk factors in men33; by contrast, the presence of CAC in women improves risk prediction of CVD in traditionally defined low-risk women34 and in older women but not older men.33 These findings offer pathophysiological insight into why men are more likely than women to develop typical rather than atypical forms of both subclinical as well as clinical atherosclerotic disease across the lifespan.
Sex differences in vascular ageing patterns appear to underlie the extent to which men versus women tend to present with typical versus atypical atherosclerotic disease (figure 2). Classic coronary artery disease (CAD) symptoms and diagnostic findings are relatively consistent across the lifespan in men but vary with age in women. In women, the prevalence of typical obstructive coronary disease is low prior to menopause and then increases dramatically after age 50, affecting only 14% of women below age 45 and up to 79% of women age 75 or older.35 By contrast, non-obstructive CAD is substantially more common in women than in men throughout life and especially in younger age. In the presence of non-obstructive CAD, women are more likely to have microvascular and/or endothelial dysfunction, in addition to conditions such as epicardial and microvascular spasm, myocardial bridging and conduit vessel stiffening, all of which can lead to myocardial ischaemia.36 Women have also been found to have thicker arteriolar walls than men in the presence of CAD.37 Accordingly, women are more likely than men to experience angina, ischaemia and acute coronary syndrome in the presence of non-obstructive CAD.36 It has been proposed that both microvascular disease and epicardial atherosclerosis originate from arterial intimal injury but develop preferentially in women versus men based on sex differences in vascular remodeling and reactivity related to hormonal exposures and risk factor clustering.38 The relatively greater prevalence of non-obstructive CAD in women, which is less easily diagnosed and treated than obstructive CAD,36 ,39 may well contribute to the consistently reported worse outcomes related to acute coronary syndromes in women than in men40. Although men are more frequently diagnosed with acute coronary syndromes each year,41 women have an almost double mortality rate at 30 days42 and a 25% greater odds of having an adverse cardiac event at 6 months.43 Notably, women up to 55 years old represent a major demographic in whom CAD mortality has not markedly declined in recent decades.44
Beyond the menopausal transition
The more pronounced age-related cardiovascular risk seen in postmenopausal compared with premenopausal women is commonly attributed to the midlife withdrawal of endogenous sex steroids, often referred to as the ‘menopausal transition’. However, recent experimental and population data suggest that hormonal changes alone are unlikely to completely explain observed sex differences in cardiovascular presentations and outcomes. On the one hand, the potential relationship between endogenous oestrogen and cardiovascular disease is supported by several lines of evidence45: the existence of oestrogen receptors in the myocardium, vascular endothelium, smooth muscle and adventitial cells46; genomic and non-genomic effects of oestrogen on endothelial and vascular smooth muscle cells47 and an inverse association between brachial artery flow-mediated dilation and years since menopause48 coupled with a positive association between serum E2 levels and brachial artery flow-mediated dilation in postmenopausal women.49 On the other hand, only a limited number of longitudinal studies have investigated associations between circulating sex steroids, sex hormone binding globulin levels and incident CAD with variable results.44 ,50 In addition, a meta-analysis of observational studies found no convincing associations between postmenopausal status or average age of menopause and outcomes.51
The extent to which menopause versus biological ageing processes contribute to age-related cardiovascular risk in women remains a subject of ongoing debate. The question is methodologically challenging to investigate given the concurrent timing and interrelatedness of these two processes.52 Data from several large-scale transition and cohort studies offer some insights. In the Study of Women Across the Nation, only select lipid measures including LDL cholesterol and apolipoprotein B changed within a year of a woman's last menstrual period; common cardiovascular risk factors changed in association with age, but not with menopause.53 Similarly, data from the Framingham Heart Study have suggested that cardiovascular risk status, represented by weight, blood pressure and total cholesterol level, influences age at menopause and not vice versa.54 Nonetheless, it should be recognised that risk factor levels in women can indeed change around the time of menopause, and in some cases dramatically,55 likely related to the combination of chronologic ageing and the menopausal transition. Thus, irrespective of the ultimate cause, women should be made aware that their cardiovascular risk is likely to increase around the time of menopause and women should be counselled regarding the importance of risk factor modification and therapeutic lifestyle changes. Risk factor monitoring should be prioritised to identify women who may benefit from pharmacologic risk factor management.
With respect to the possible role of menopause in conferring cardiovascular risk, additional insights can be gained from examining age-based trends in the incidence of breast cancer, a condition that is biologically more clearly related to endogenous oestrogen levels. The Women's Health Initiative (WHI) demonstrated that breast cancer incidence and related mortality were lower for postmenopausal women who took oestrogen alone as compared with placebo,56 ,57 regardless of when hormone therapy was initiated. By contrast, major trials of hormone therapy in menopause including the WHI have demonstrated no obvious reduction in either subclinical CVD58 or overt CVD outcomes,56 ,59 ,60 although with some evidence suggesting that hormone therapy initiated at an earlier versus later age could confer more protective than harmful cardiovascular effects.61 In fact, a fair amount of data support the hypothesis that the cardioprotective effects of hormone therapy are time dependent and more beneficial than harmful if started in the perimenopausal or early postmenopausal period rather than late after menopause. Accordingly, experimental and physiology data also suggest differential effects of oestrogen on vascular reactivity depending on when therapy is initiated with respect to age and menopausal status.62
Population studies also offer additional insights regarding the contrasting patterns of age-related cardiovascular versus breast cancer risk. Two decades ago, Elizabeth Barrett-Connor analysed mortality statistics and suggested that menopause itself has no discernible effect on the exponential increase in coronary death with age, given that coronary death rates in women do not markedly accelerate after menopause, in contrast to the relatively abrupt drop in deaths attributable to breast cancer.63 Updated national mortality data from the US Centers for Disease Control continue to support this observation (figure 4),64 where the apparent perimenopausal increase in CAD mortality in women may actually be more reflective of a relative decrease in CAD mortality in men, beginning around age 45. Thus, it has been suggested that the observed gender gap is not primarily due to oestrogen deficiency but instead due to CAD mortality rates that tend to decrease in men while continuing to steadily rise in women with advancing age.65 Importantly, observational studies have noted that the sexual dimorphism in both subclinical and clinical cardiovascular phenotypes exists in prepuberty,66–68 suggesting that intrinsic non-hormonal factors acting throughout the life course may play a more important role than midlife hormonal shifts, with respect to sex differences in cardiovascular risk.
Conclusions
Over the past two decades, tremendous progress has been made in identifying and narrowing the gaps in cardiovascular outcomes observed between men and women. Despite this progress, general understanding of how and why manifestations of cardiovascular disease differ between the sexes remains limited. Evidence to date indicates that the development and progression of cardiovascular disease varies between women and men due to both intrinsic biological sex differences as well as sex differences in how age-related changes in cardiac and vascular anatomy and physiology progress over the life course. Although men are more susceptible to typical subclinical and clinical vascular changes beginning earlier in life, women are more at risk for atypical vascular disease in general in addition to more accelerated age-related vascular changes at midlife—predisposing them to both typical and atypical manifestations in older age. Given the acceleration in arterial stiffness and subclinical atherosclerosis that can be seen in perimenopausal women, in particular, coupled with changes in cardiac remodeling and diastolic function, a key target for risk factor modification is hypertension. Ideally, hypertension or even prehypertension should be targeted for treatment well prior to the onset of menopause, if present. Targeting premature chronic elevations in arterial pressure and afterload may, in turn, prove to be the most efficacious strategy for preventing HFPEF in older women as well as in older men. It is well recognised that hormone therapy should not be used for long-term chronic disease prevention, as it may increase cardiovascular risk in some older women and especially women farther out from menopause. As it turns out, avoidance of hormone therapy in ageing women is not likely to represent a substantially missed opportunity. While considerable evidence has pointed to the influence of the menopausal withdrawal of endogenous oestrogen on the increase in age-related cardiovascular risk in postmenopausal compared with premenopausal women, chronologic ageing processes acting on top of inherent biological differences between men and women likely play a more important role.
Acknowledgments
We acknowledge that references to the work of many investigators were omitted due to the word limit for this manuscript.
References
Footnotes
Contributors AAM: drafted the work and revised it critically for important intellectual content. SC: drafted the work and revised it critically for important intellectual content.
Funding This work was supported by the Ellison Foundation (SC) and NIH/NHLBI grant R00HL107642 (SC).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.