Article Text

Abstract
Objective Acute heart failure (AHF) is associated with high mortality and morbidity. Trimethylamine N-oxide (TMAO), a gut-derived metabolite, has reported association with mortality risk in chronic HF but this association in AHF is still unknown. The present study investigated TMAO in patients admitted to hospital with AHF, and association of circulating levels with prognosis.
Methods In total, 972 plasma samples were analysed for TMAO concentration by liquid chromatography-mass spectrometry. Associations with in-hospital mortality (72 events), all-cause mortality (death, 268 events) and a composite of death or rehospitalisation due to HF (death/HF, 384 events) at 1 year were examined.
Results TMAO improved risk stratification for in-hospital mortality in combination with current clinical scorings (OR≥1.13, p≤0.014). TMAO tertile analyses reported a graded risk in adverse outcome within 1 year (OR≥1.61, p≤0.004) and improved outcome prediction when stratified as none, one or both biomarker(s) elevated in combination with N-terminal pro B-type natriuretic peptide (NT-proBNP) (OR≥2.15, p≤0.007). TMAO was independently predictive for death and death/HF when corrected for cardiac risk factors (HR≥1.16, p≤0.037); however, this ability was weakened when indices of renal function were included, possibly due to multicollinearity.
Conclusions TMAO contributed additional information on patient stratification for in-hospital mortality of AHF admissions using available clinical scores that include renal indices. Furthermore, elevated levels were associated with poor prognosis at 1 year and combination of TMAO and NT-proBNP provided additional prognostic information. TMAO was a univariate predictor of death and death/HF, and remained an independent predictor until adjusted for renal confounders.
Statistics from Altmetric.com
Introduction
Heart failure (HF) is one of the most common heart conditions, especially in the elderly, and has a high morbidity and mortality.1 More than 23 million people worldwide suffer from HF,2 and approximately 50% of HF events lead to death within 5 years.3 A multitude of factors and pathways regulate the development of this condition (eg, neurohormonal regulation, mechanical stress/hypertension and so on) as a (mal)adaptation/remodelling response of the heart to intrinsic and extrinsic stresses.4
Recent studies have identified a hitherto unknown interaction of the gut microbiome with cardiovascular disease.5 The bacterial flora, which shows heterogeneity between individuals with seasonal and dietary influences,6 generates metabolites from dietary nutrients.7 One pathway involves carnitine, a large nutritional component of red meat, which is digested by bacteria into the downstream metabolite, trimethylamine N-oxide (TMAO). TMAO is formed when bacteria cleave trimethylamine from the carnitine molecule, which is reabsorbed into the bloodstream and converted to TMAO in the liver by flavin-containing monooxygenases.8
Investigations of TMAO in heart disease have shown an association of elevated levels with coronary artery disease,9 promotion of atherosclerotic plaque formation,10 renal fibrosis11 and the prolongation of the hypertensive effect of angiotensin II.12 In addition, poorer prognosis (at 5 years) has been reported in chronic HF (CHF) patients with elevated levels of circulating TMAO.13 Thus, there seems to be an association between increased circulating levels of the gut-derived metabolite and progression of cardiovascular conditions. To our knowledge, the role of TMAO in acute HF (AHF) remains unaddressed. The present study, therefore, sought to investigate whether plasma TMAO concentrations show an association with AHF and provide additional information for assessment of prognosis of the condition.
Methods
Study population
Nine hundred and seventy-two patients with AHF were admitted to the University Hospitals of Leicester, UK between February 2006 and August 2011. Each patient consented (written and informed) to have blood samples taken and outcomes surveyed. This study complied with the Declaration of Helsinki and was approved by the local ethics committee. Diagnosis of AHF was made on the basis of progressive worsening or new onset of shortness of breath along with clinical signs of pulmonary oedema, peripheral oedema or elevated jugular venous pressure.14 Exclusion criteria included previous history of cancer or renal replacement therapy; any surgical procedure within the previous month; presence of cardiogenic shock, sepsis, pneumonia; acute coronary syndromes (ACS); and inability to consent (eg, dementia). Where echocardiograms were performed, patients were not excluded on values of preserved/reduced ejection fraction.
The primary endpoints were all-cause mortality (death) and a composite of death or rehospitalisation due to HF (death/HF) at 1 year, as obtained from hospital records. All surviving patients were followed up for at least 1 year after initial hospitalisation, with a cut-off at 1 year implemented for the data in this report. All inclusion and endpoint determinations were performed by an independent cardiologist. In cases where the patient had multiple events, the time to first event was counted as the outcome. The simplified modified diet in renal disease formula was used to estimate glomerular filtration rate (GFR).15
Sample collection
Venepuncture was performed in recumbent patients within the initial 24 h period after admission to hospital with AHF. Blood was collected in prechilled tubes containing EDTA and aprotonin, and plasma was separated by centrifugation at 1500g for 20 min at 4°C. Plasma was aliquoted and stored at −80°C until analysis. At the time of analysis, samples were defrosted at room temperature and analysed immediately after preparation.
TMAO and other biomarker measurements
Plasma TMAO was extracted using stable-isotope dilution and analysed by ultraperformance liquid chromatography-mass spectrometry, with previously reported techniques.16 A brief explanation of these methods is described in the online supplementary material. N-terminal pro B-type natriuretic peptide (NT-proBNP) was measured in all patients using a sandwich immunoassay as described previously.17
Statistical analyses
Statistical analyses were performed using IBM SPSS Statistics (V.22, IBM Corp, Armonk, New York, USA) and Stata (V.14, College Station, Texas, USA). Patient demographics were compared using the Mann–Whitney independent U test for continuous variables and χ2 tests for categorical variables, after stratification by TMAO levels. Spearman's correlations were performed on TMAO values and continuous variables. Cox proportional hazard analyses were used to identify the independent predictors of death and death/HF. Multivariate models were created with and without the inclusion of markers of renal function. TMAO and NT-proBNP levels were log transformed, and normalised to 1 SD, so that HRs refer to the Z-transformed variables. Kaplan–Meier survival curves were generated to visualise the relationship between TMAO and the outcome of death/HF. Mantel–Cox log rank tests were used to assess the significance of the stratification of using tertiles of TMAO and the relationship of above-median and below-median levels of TMAO and NT-proBNP in combination. Additional Kaplan–Meier survival curves were generated to test the adverse outcome relationships of TMAO levels and patients with and without de novo HF. To test the predictive power of TMAO for in-hospital mortality, binary logistic regression analyses were conducted and included the ADHERE, OPTIMIZE-HF or GWTG-HF score.18–20 The ADHERE score was categorised against the first (reference) grouping and patients were assigned to risk groups 1 (lowest) to 5 (highest) using the ADHERE registry model. In addition, the ADHERE score probability was calculated as a continuous variable from the following formula for log odds mortality18: −0.0212×blood urea nitrogen−0.0192×systolic blood pressure (BP)+0.0131×heart rate+0.0288×age−4.72, and Z-transformed for use in analyses. OPTIMIZE-HF and GWTG-HF data were Z-transformed for analyses. Additional logistic regression calculations were performed for each of the clinical risk score components listed individually, with the addition of TMAO. Comparison of receiver operator characteristic (ROC) curve areas was performed by calculating the probability of outcome for each model and comparing baseline in-hospital mortality models versus those models with the addition of either NT-proBNP and/or TMAO. Reclassification analyses21 were used to assess the utility of addition of TMAO and NT-proBNP to a basic model of clinical risk scorings alone. A two-sided p value of <0.05 was deemed to be statistically significant.
Results
Patient demographics
Clinical and demographic factors are shown in table 1 for the entire cohort and further categorised to above-median and below-median TMAO levels. Analysis of trends for TMAO showed that individuals with higher levels of TMAO were more likely to be older, have reduced renal function, decreased heart rate, BP and haemoglobin levels, increased levels of NT-proBNP and potassium, and reduced left ventricular ejection fraction (p≤0.038). More patients in the higher TMAO group had diabetes or previous HF, evidence of oedema or atrial fibrillation, and were in New York Heart Association (NYHA) class IV (p≤0.042).
Patient demographics at time of admission to hospital with AHF
Clinical parameters associated with TMAO
Spearman's correlation analyses were performed to assess the clinical correlates of TMAO. Spearman's rank correlation coefficients (rs) showed that TMAO was significantly correlated to age (0.230), estimated GFR (eGFR) (−0.528), blood urea (0.529), serum creatinine (0.515), NT-proBNP (0.207), systolic BP (−0.110) and heart rate (−0.108, all p's <0.0005).
A general linear model for independent predictors of log TMAO levels indicated that the most significant predictors of TMAO were age, blood urea and eGFR, with smaller contributions from past history of diabetes, smoking status, atrial fibrillation and NYHA class (table 2). The general linear model reported that the variation of TMAO as explained by all factors was 32.4%.
General linear model showing independent predictors of log-transformed TMAO levels, with coefficients reported for 2000 bootstrapped samples
Plasma TMAO levels as a predictor of death/HF at 1 year
Cox survival analyses, including traditional cardiovascular risk factors and variables that independently predict TMAO levels, for the primary endpoint of death/HF at 1 year were produced (figure 1A, B). TMAO was a univariate predictor of death/HF (HR (95% CI) 1.33 (1.20 to 1.46), p<0.0005). As TMAO is strongly associated with renal function, with eGFR and urea recording variance inflation factors (VIFs) of 16.2 and 7.9, respectively, multivariate analyses were performed with and without the inclusion of these confounding factors, which may show collinearity with TMAO. In multivariate analyses for death/HF without correction for renal function, independent predictors included age, de novo HF and past history of diabetes, NYHA class, systolic BP, heart rate, respiratory rate and NT-proBNP. TMAO also showed independent predictive value (HR 1.18 (1.05 to 1.33), p=0.005) (figure 1A). When eGFR and urea were added to the model, TMAO was no longer able to independently predict death/HF, indicating a strong confounding influence from biomarkers of renal function (figure 1B). Data modelling on a subset of patients, with the addition of cardiac troponin, can be seen in online supplementary tables S1 and S2 (note that cardiac troponin was available for 503 patients only). The findings on TMAO were similar to those when troponin was excluded.
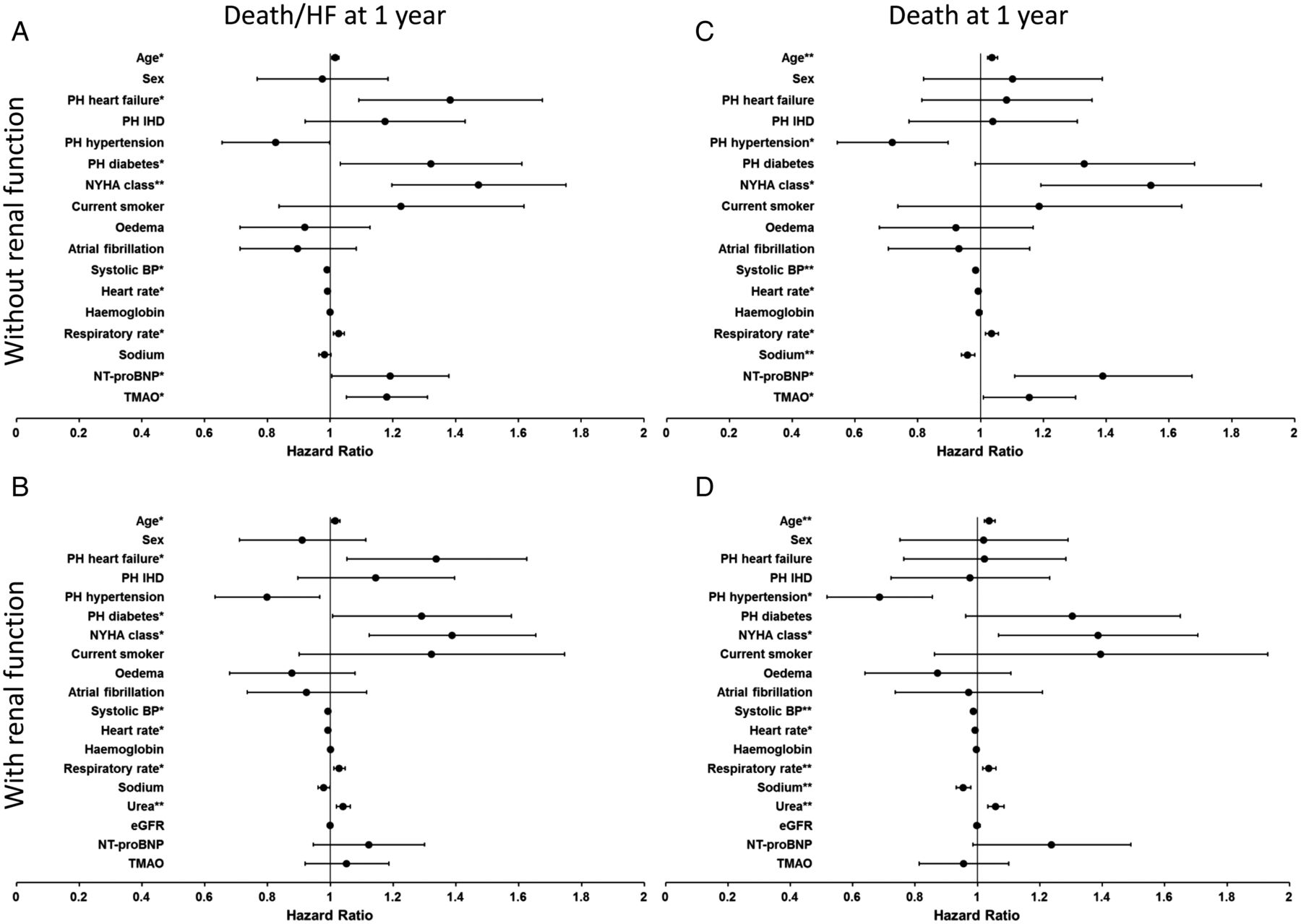
Forest plots to show Cox HRs (black dots) and 95% CIs (horizontal bars) for cardiac risk factors. Multivariate models excluding (top) and including (bottom) renal function for death or HF rehospitalisation (death/HF, left) and death at 1 year (right) are shown. BP, blood pressure; eGFR, estimated glomerular filtration rate; HF, heart failure; IHD, ischaemic heart disease; NT-proBNP, N-terminal pro B-type natriuretic peptide; NYHA, New York Heart Association; PH, past history; TMAO, trimethylamine N-oxide; *p<0.05; **p<0.0005.
Kaplan–Meier survival analysis performed on death/HF rates in TMAO tertiles (figure 2A) showed that the highest tertile was different from the lowest (p<0.0005) and middle (p=0.04), and for the middle tertile to be different from the lowest (p=0.004). The TMAO values for each tertile and the increase in OR were as follows: lowest tertile (range (median)) 0.5–4.0 (2.9) µmol/L; middle tertile, 4.1–8.1 (5.6) µmol/L (OR (95% CI) 1.61 (1.17 to 2.20), p=0.004) and highest tertile, 8.2–151.5 (14.2) µmol/L (OR 2.12 (1.54 to 2.93), p<0.0005).

Kaplan–Meier survival analysis for death or rehospitalisation due to heart failure (death/heart failure (HF)) stratified by (A) tertiles of trimethylamine N-oxide (TMAO) values, and (B) combinations of TMAO and N-terminal pro B-type natriuretic peptide (NT-proBNP) reporting none, one or both biomarkers elevated.
When patients were categorised according to below-median or above-median levels of TMAO and NT-proBNP, there was a graded increase in death/HF depending on risk groups: group with TMAO and NT-proBNP less than median versus group with either TMAO or NT-proBNP greater than median (OR 2.15 (1.59 to 2.91), p<0.0005); and group with both TMAO and NT-proBNP greater than median (OR 3.14 (2.18 to 4.50), p<0.0005). The group with both biomarkers elevated was different from all other groups (p<0.0005, figure 2B), and the group with either biomarker elevated differed from the group with neither elevated (p=0.007). No differences were reported between high TMAO with low NT-proBNP, and low TMAO with high NT-proBNP (data not shown). Patients were further stratified into four groups, dependent on high or low TMAO and whether they suffered recurrent or de novo HF. No differences were seen in survival curves for death/HF between any groups (p≥0.144) (see online supplementary figure S1).
Plasma TMAO levels as a predictor of death at 1 year
Univariate analysis showed that TMAO was a predictor of death (HR 1.35 (1.21 to 1.51), p<0.0005). In multivariate analyses, without correction for renal function, independent predictors included age, past history of hypertension, NYHA class, systolic BP, heart rate, respiratory rate, sodium and NT-proBNP. TMAO also showed independent predictive value (HR 1.16 (1.01 to 1.33), p=0.037) (figure 1C). When eGFR and urea were added to the model, TMAO was no longer able to independently predict the outcome for death at 1 year (figure 1D). When stratifying patients by high/low TMAO and recurrent/de novo HF, differences in survival curves were reported with elevated TMAO and de novo HF versus low TMAO with recurrent HF (adjusted p=0.048) (see online supplementary figure S2). Multivariate models in a subset with the addition of cardiac troponin can be seen in online supplementary tables S3 and S4.
Plasma TMAO levels as a predictor of in-hospital mortality
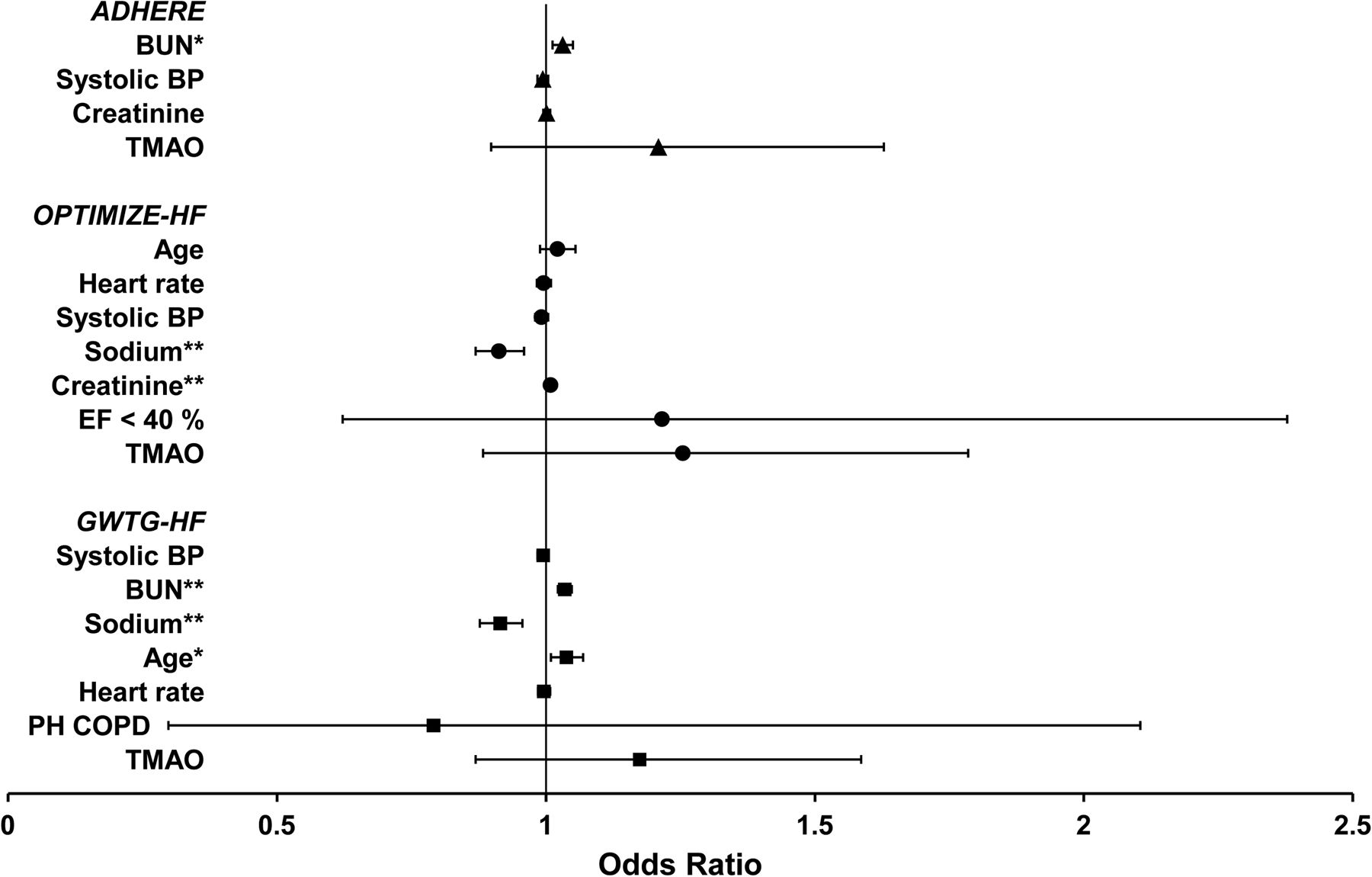
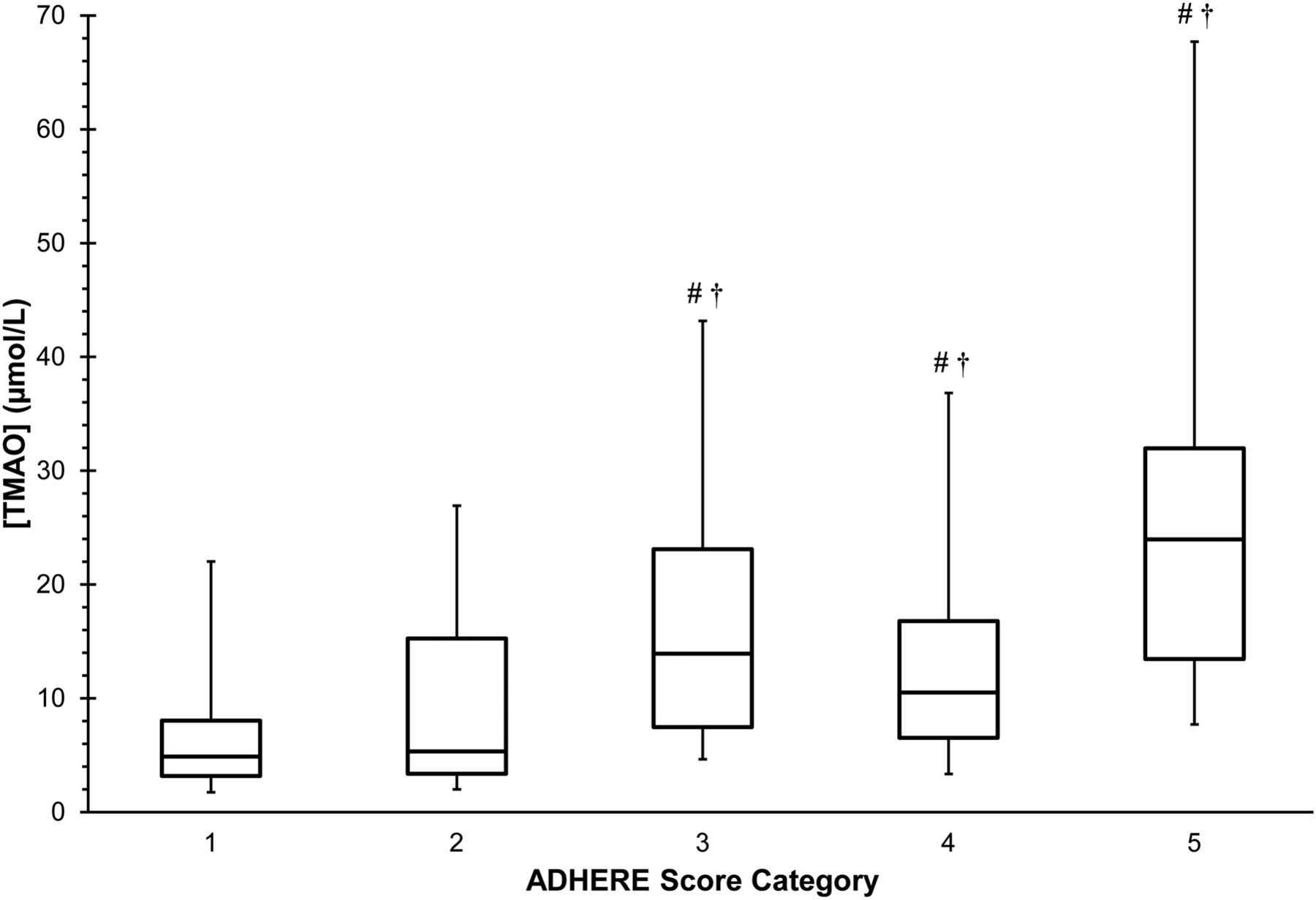
Analyses were performed to determine the added value of TMAO, alongside NT-proBNP, with clinical risk scores as either a categorical (ADHERE) or continuous variable (ADHERE, OPTIMIZE-HF and GWTG-HF). TMAO levels, stratified by ADHERE categorical score, were elevated in groups 3–5 and are shown in figure 3. TMAO was an independent predictor with all three clinical risk scores (OR≥1.13, p≤0.012). Interestingly, NT-proBNP was not an independent predictor (see online supplementary table S5). When TMAO was added to a base model of the clinical risk scores presented as their individual components, TMAO was no longer able to independently predict in-hospital mortality, with a strong influence from biomarkers of renal function (figure 4).

Box and whisker plot to show the distribution of trimethylamine N-oxide (TMAO) across in patients stratified by ADHERE score18 grouping. Boxes indicate median and IQR, and whiskers indicate 5th and 95th percentiles. #p<0.0005 when compared with group 1; †p≤0.001 when compared with group 2.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plots to show binary logistic ORs (dots) and 95% CIs (horizontal bars) for cardiac risk factors for multivariate models for the individual components of in-hospital mortality prediction algorithms of ADHERE (triangles),18 OPTIMIZE-HF (circles)19 and GWTG-HF (squares)20 registries with the addition of TMAO. BP, blood pressure; BUN, blood urea nitrogen; COPD, chronic obstructive pulmonary disease; EF, ejection fraction; PH, past history; TMAO, trimethylamine N-oxide; *p<0.05; **p<0.0005.
Reclassification analyses, using the continuous net reclassification improvement index (table 3), showed similar findings. NT-proBNP did not improve reclassification, whereas TMAO did by a down-classification of risk in those without endpoints (p<0.0005). Further reclassification analyses were performed using the three clinical variables in the ADHERE scoring system (blood urea nitrogen, systolic BP and creatinine) and the data reported comparable findings to those obtained using the ADHERE log odds mortality calculations (see online supplementary table S6).
Reclassification analysis, for the endpoint of in-hospital mortality, using continuous reclassification showing the net reclassification index (NRI) of adding N-terminal pro B-type natriuretic peptide (NT-proBNP) or trimethylamine N-oxide (TMAO) to the classification using ADHERE (left), OPTIMIZE-HF (centre) and GWTG-HF (right) scoring only, and for adding TMAO to the classification using the clinical risk algorithm scoring with NT-proBNP
Discussion
The present study shows that the gut-derived metabolite, TMAO, demonstrates an association of circulating levels with AHF, and to be a predictive biomarker for death and death/HF at 1 year. Inclusion of markers of renal function caused TMAO to lose independent predictive ability, possibly due to multicollinearity as TMAO was significantly correlated to both urea and eGFR. Furthermore, TMAO improved risk stratification for in-hospital mortality in combination with current clinical risk scoring methods. TMAO had been previously reported to show independent association with adverse outcomes in stable HF patients at 5 years.13 Collectively, we find that TMAO is additive in the prediction of death and death/HF within 1 year, when renal function is excluded. However, TMAO was additive in the prediction of in-hospital mortality in patients with AHF when using clinical risk scores that incorporate renal indices.
TMAO further strengthened the prediction of death/HF at 1 year when combined with NT-proBNP. Patients with elevated levels in both markers were at the highest risk of death/HF, with a graded risk seen above those with one, or neither elevated. Combining these two circulatory analytes may provide useful prognostic information in clinical assessment of AHF as previously demonstrated in stable HF.13 As NT-proBNP reflects neurohormonal regulation of HF, and TMAO the involvement of the gut microbiome, it is likely that these biomarkers reflect different and independent mechanistic contributions within the complexity of HF.
When used in combination with the clinical risk algorithms developed for in-hospital mortality, TMAO was able to independently predict in-hospital mortality for patients being admitted with AHF. Interestingly, NT-proBNP did not add to in-hospital mortality prediction for this cohort, and even significantly down- or up-classified risk in those with or without events when using the OPTIMIZE-HF score. When added to a baseline model consisting of both the clinical risk score and NT-proBNP, TMAO was able to improve the stratification and refine classification of mortality risk by predominantly down-classifying those without endpoints. Addition of TMAO to the base model of the clinical risk scores did not increase the ROC areas. However, it has been previously demonstrated that where comparisons of the ROC area report as insignificant, reclassification analyses may offer greater sensitivity in highlighting an improvement for the inclusion of an additional variable.22 Further improvements in sensitivity have been described when using continuous category-free reclassification,21 as performed with these data. However, in contrast, arguments have been presented to show oversensitivity in net reclassification analyses.23 Interestingly, when the percentage contribution to total in-hospital patient mortality was assessed, elevated TMAO was attributable to 75% of in-hospital deaths, whereas elevated NT-proBNP was only 51%. For those deaths with elevated NT-proBNP, 78% of these patients also reported elevated TMAO, therefore supporting the association of elevated levels of TMAO with increased in-hospital mortality (see online supplementary figure S3). This finding might suggest that the gut microbiome contributes more than neurohormonal regulation to short-term outcome in AHF.
The inverse relationship of TMAO and renal function reported in this and previous work13 may partially explain the link with poor prognosis, although TMAO may have additional effects independent of this relationship since the clinical risk scores have measures of renal function incorporated. Association of TMAO with prognostic ability for AHF was not as strong as seen previously with stable HF.13 Although the mechanistic underpinnings of this are not clear, these findings might suggest that there is less contribution of the gut microbiome to AHF than CHF. The loss of independent predictive value of TMAO when renal indices were included must be interpreted with caution. The high VIF values of urea and eGFR, in relation to TMAO, may have reduced the level of statistical significance of TMAO in modelling due to multicollinearity. Correction for eGFR has been used in previous HF cohorts,13 ,24 ,25 but no data currently report how levels of blood urea affect the multivariate prediction models in CHF or ischaemic heart disease. Sample collections for TMAO analyses were not strictly time-controlled due to emergency admission procedures. Urinary levels are subject to time variation,26 although time variability in blood is currently unknown. Other factors (eg, time since last meal or urination) may alter the relationship of TMAO to renal metabolites and these data would be additive in future experiments.
Although a rise in TMAO has been linked to increased intake of carnitine,10 this is associated with a pro-atherosclerotic effect that is less likely to be a reason for adverse outcome in this cohort as ACS were excluded. However, the onset of renal fibrosis with elevated TMAO levels11 may provide a more plausible link to the pathophysiology of AHF cases. TMAO has been shown to be effectively removed from the circulation by dialysis in chronic kidney disease patients,27 and therefore a reduction in renal function is a likely cause for the increase in plasma TMAO concentrations. Mechanistically, increased TMAO may induce renal fibrosis and, therefore, cause further reduction in renal function. Combined with increased permeability of the gut epithelium associated with intestinal congestion in HF,28 this may lead to rapid circulatory rises in gut-derived metabolites such as TMAO. Circulating TMAO may, therefore, be important in patients with AHF and downregulation of levels may potentially aid in the suppression of further renal impairment, and ultimately a reduction in adverse outcome. Data to confirm these links are not currently available and would provide great insight into the role of TMAO measurements in this population.
In conclusion, TMAO levels contribute to risk prediction models for in-hospital mortality, associate with poor prognosis at 1 year and strongly associate with renal dysfunction in patients with AHF. A larger, multicentre validation cohort with extended clinical data would provide additional information and strengthen the understanding for the prognostic use of TMAO following admission with AHF.
Key messages
What is already known on this subject?
Elevated levels of trimethylamine N-oxide (TMAO), a gut-derived metabolite, have shown association with cardiovascular disease and report poor survival statistics in stable heart failure patients.
What might this study add?
TMAO contributes to risk prediction of in-hospital mortality in acute heart failure (AHF) when combined with current clinical risk scores that include adjustment for renal function (OR ≥1.13, p≤0.014). Reclassification analyses reported an improvement for the combination of TMAO with clinical risk scores by down-classifying those who survived the hospital admission period (net reclassification index ≥26.1, p≤0.033).
How might this impact on clinical practice?
As routine clinical measurements expand and gut-derived metabolites are being considered as potential biomarkers, we report that measurements of TMAO for AHF admissions may benefit clinicians when categorising patients for short-term risk of serious adverse events.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
TS and LMH contributed equally.
Twitter Follow Liam Heaney at @HeaneyLM
Contributors TS—design of work, interpretation of data, drafting and critical revision of manuscript, approval of the final version of the manuscript. LMH—design of work, analysis of samples, acquisition and interpretation of data, drafting of the manuscript, approval of the final version of the manuscript. SSB—interpretation of data, drafting of the manuscript, approval of the final version of the manuscript. DJLJ—design of work, analysis of samples, acquisition and interpretation of data, critical revision of the manuscript, approval of the final version of the manuscript. LLN—design of the work, acquisition of the clinical samples, analysis and interpretation of the data, drafting and critical revision of the manuscript, approval of the final version of the manuscript. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This work was supported by the John and Lucille van Geest Foundation and the National Institute for Health Research Leicester Cardiovascular Biomedical Research Unit.
Competing interests None declared.
Ethics approval National Research Ethics Service (NRES), UK.
Provenance and peer review Not commissioned; externally peer reviewed.