Article Text

Abstract
Objective New imaging techniques have permitted the detection of subclinical LV dysfunction (LVD) in up to half of patients with type 2 diabetes mellitus (DM) with a normal EF. However, the connection between early LVD and prognosis is unclear. This study aimed to define the long-term outcome of LVD associated with type 2 DM.
Methods In this prospective cohort study, 230 asymptomatic patients with type 2 DM underwent measurement of global longitudinal 2D strain (GLS) for detection of LVD and were followed for up to 10 years. All subjects had normal EF (≥50%) and no evidence of coronary artery disease at recruitment. Outcome data were obtained through centralised state-wide death and hospital admission registries. The primary endpoint was all-cause mortality and hospitalisation.
Results On study entry, almost half (45%) of the cohort had evidence of LVD as detected by GLS. Over a median follow-up of 7.4±2.6 years (range 0.6–9.7 years), 68 patients (30%) met the primary endpoint (LVD: 37%; normal LV function: 24%). GLS was independently associated with the primary endpoint (HR=1.10; p=0.04), as was systolic blood pressure (HR=1.02; p<0.001) and levels of glycosylated haemoglobin (HR=1.28; p=0.011). Patients with LVD had significantly worse outcome than those without (χ2=4.73; p=0.030).
Conclusions Subclinical LVD is common in asymptomatic patients with type 2 DM, is readily detectable by GLS imaging and is independently associated with adverse outcome.
Trial registration number Australian and New Zealand Clinical Trials Registry (ACTRN12612001178831).
Statistics from Altmetric.com
Background
Worldwide, diabetes mellitus (DM) accounts for 8.4% of all-cause mortality in adults, with up to half attributable to the accelerated development of cardiovascular disease.1 ,2 The development of heart failure in patients with DM was demonstrated in the Framingham studies, where the risk was increased twofold for men and fivefold for women.3 DM is an independent predictor of mortality and morbidity regardless of LVEF.4 Importantly, the presence of DM in patients with heart failure with normal EF appears to confer greater risk than patients without DM and a low EF.4
Despite its role as the fundamental evaluation of systolic function for over four decades, LVEF is less sensitive for detecting early myocardial disease than newer echocardiographic techniques.5 Patients with DM often have evidence of subclinical diastolic and systolic dysfunction by tissue Doppler imaging, despite having normal EF.6–9 In contrast to EF, 2D global longitudinal strain (GLS) measured by myocardial deformation imaging is more sensitive for the detection of subclinical systolic LV dysfunction (LVD).9–11 LVD is common, even in asymptomatic patients, with recent data suggesting that it is present in up to half of patients with type 2 DM.12–14 Importantly, strain imaging is sensitive for identifying the myocardial dysfunction15 and myocardial fibrosis16 associated with LVD in patients with type 2 DM.
Detection of early LVD may confer adverse prognosis;17 however, the long-term outcome associated with impaired GLS is not known. Early detection and management of diabetic heart disease may mitigate some of the cardiovascular risks associated with DM. The aim of this study is to report long-term outcome in patients with subclinical LVD and to identify potential modifiers of risk in asymptomatic patients with type 2 DM.
Methods
Patient selection and clinical assessment
We prospectively recruited a cohort of 249 patients with type 2 DM between October 2002 and March 2006. Patients recruited from hospital clinics and by advertisement were included if they had a normal EF (≥50%), a negative exercise stress echocardiogram for inducible ischaemia and/or normal coronary angiogram, no known or existing ischaemic heart disease, in sinus rhythm and without valvular disease greater than mild in severity. All patients signed informed consent on recruitment, and underwent measurement of waist and hip circumferences, height, weight and calculation of body mass index (BMI). Blood pressure (BP) was recorded as the average of three measurements taken by mercury sphygmomanometry. A fasting blood test was performed to determine serum glucose, glycosylated haemoglobin (HbA1c), lipid profile, electrolytes and renal function. Exercise capacity was determined by expired gas analysis and treadmill metabolic equivalents (METs) during the baseline exercise test.
Echocardiography
All patients underwent a standard resting echocardiogram for assessment of LV systolic and diastolic function and valvular competence. Echocardiography was performed by experienced sonographers using a 3.5 MHz transducer on standard cardiac ultrasound machines (Vivid 7 or e9, General Electric Medical Systems, Milwaukee, Wisconsin, USA). Images were recorded in raw data format and stored for offline analysis. EF was calculated by Simpson's biplane method using end-diastolic and end-systolic volumes measured in apical two-chamber and four-chamber views.18 LV mass was calculated by standard methods and indexed to height2.7.18 Only patients with a normal EF (i.e. ≥50%) and no evidence of wall motion abnormalities at rest or exercise were included in this study. Diastolic function was assessed by standard criteria19 using transmitral flow and tissue velocities measured during systole (Sm), and early (Em) and late (Am) diastole. LV filling pressure was considered raised if the E/Em ratio was >15.
Myocardial deformation imaging
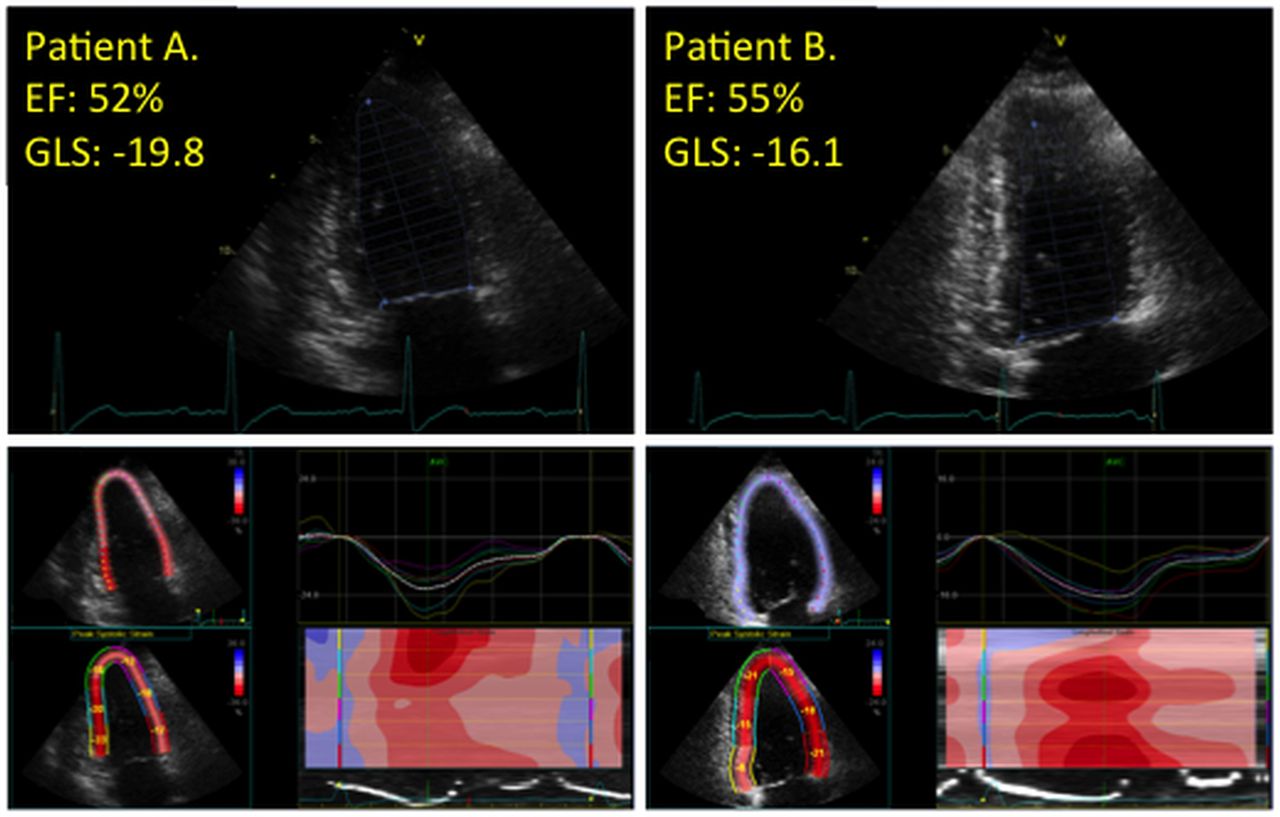
GLS and strain rate were measured offline, from saved cine-loops using standard software (EchoPac v9, General Electric Medical Systems, Milwaukee, Wisconsin, USA). 2D images were used to trace endocardial borders from the three apical views. GLS was calculated as the average of 18 segments. If segments could not be successfully tracked, they were excluded from the analysis. All measurements were completed by a single operator, who was blind to clinical and outcome data. Reproducibility of this technique by our group has been previously reported.5 The presence of LVD was defined using normal values published in a recent large meta-analysis of strain. The mean GLS in normal subjects was −19.7%, with a lower 95% CI of −18.9%.20 Because all patients were free of ischaemic heart disease, untreated hypertension, valvular disease and others causes of cardiomyopathy, those with a GLS more positive than the −18.9% threshold (i.e. closer to zero) were considered to have LVD. Examples of this technique, with comparison to EF, are provided in figure 1.

Example measurements of EF and 2D strain (two-chamber views). The two-chamber images are combined with four-chamber and apical long-axis views to generate global longitudinal strain. Despite having similar EFs, patient A (left) has normal values of strain whereas patient B (right) has evidence of subclinical LV dysfunction. GLS, global longitudinal strain.
Outcomes
Prognostic data were obtained through a state-wide data-linkage service. The International Classification of Diseases (V.10) was used to categorise clinical endpoints over the follow-up period from October 2002 to June 2012. Records of hospital admission were obtained through the state Hospital Admitted Patient Data Collection, whereas records of deaths were obtained through the state Registrar General linkage dataset. The primary endpoint for the study was all-cause mortality and hospitalisation. The secondary endpoint was the individual outcome of all-cause hospitalisation. Where multiple admissions occurred over the follow-up period, the first event was recorded. The principal diagnosis, recorded at the time of hospital admission by the attending physician, was considered the reason for hospitalisation.
Statistical analysis
Statistical differences between groups were calculated by Student's t-test for continuous variables and by χ2 test for categorical variables. Univariate Cox regression analysis was used to determine predictors of the primary endpoint. A backward-conditional Cox proportional hazards multivariate model was then used to determine independent correlates and reported as HR with 95% CIs. Variables were selected for entry into the model if they met univariate statistical significance of p<0.05. To evaluate the predictive power of GLS imaging, nested forward Cox models were constructed. Using the enter method, significant clinical variables were inserted into the first step of the model, followed by the significant biochemical parameters in the second step. The final step included the introduction of either GLS or EF into two separate models. The incremental value of each step was assessed using the change in model χ2 at each step. The assumption of proportional hazards was tested using Schoenfeld residuals. All data were analysed using a standard software packages (SPSS, V.21.0; SPSS, Chicago, Illinois, USA; and Stata, V.10.0, StataCorp, College Station, Texas, USA) with p<0.05 considered significant.
Results
Clinical characteristics
Clinical characteristics of 230 patients included in the final analysis are presented in table 1. At screening, 25 patients returned a positive exercise echocardiogram and were not included in the final cohort. Myocardial deformation imaging was unavailable on 19 patients due to inadequate image quality or suboptimal software tracking. The characteristics of these patients were not significantly different to the analysed cohort (p>0.05 for all). The mean age at recruitment was 56±10 years, and 55% of subjects were men. Overall, the cohort were obese (BMI 31.8±5.7 kg/m2) but normotensive (systolic BP 131±14 mm Hg). The mean exercise capacity was 6.3±1.9 METs (22.2±6.7 mL/kg/min on expired gas analysis). Mean duration of diabetes before recruitment was 6.3±6.4 years, and on enrolment into the study, 29% of patients were taking an ACE inhibitor and 4% were taking a β-blocker.
Clinical characteristics
Echocardiography and myocardial deformation
The mean EF was 66%±7% (range 50–85%) and average GLS was −18.9%±2.7% (range −10.3% to −25.9%). Accordingly, 104 patients (45%) had evidence of subclinical LVD, despite having normal EF. Those with LVD were more often men, had a higher waist-to-hip ratio, higher diastolic BP and lower Em (table 1). Based on LV geometry, there were no statistical differences between groups (normal geometry [37%; GLS=−19.3%±2.4%], concentric remodelling [39%; GLS=−18.3%±2.7%], eccentric hypertrophy [8%; GLS=−19.2%±2.7%], concentric hypertrophy [16%; GLS=−19.1%±2.8%]; p>0.1 for all). Grading of diastolic function was possible in 85% of patients. Over half had normal diastolic function (52%), and 13.5% had evidence of raised LV filling pressure (E/Em>15 or evidence of left atrial enlargement).
Outcomes
Over a median follow-up period of 7.4±2.6 years (range 0.6–9.7 years), 68 patients (29.6%) met the primary endpoint of all-cause mortality and hospitalisation (38 [37%] with LVD and 30 [24%] with normal LV function). On examination of the individual components of the primary outcome, 5 patients died and 65 were admitted to hospital. Table 2 summarises univariates and independent predictors of the primary endpoint. GLS was associated with outcome, independent of age, systolic BP, exercise capacity and HbA1c (overall model χ2=27.9; p<0.001). In this study, diastolic function was not associated with the primary endpoint.
Statistical predictors of the primary endpoint
Stepwise nested Cox models were constructed to determine the incremental value of GLS for predicting the primary endpoint. Significant clinical univariates were entered into the first step of the model (age, systolic BP and exercise capacity). Significant biochemical parameters (HbA1c) were entered into the second step, followed by GLS in the third step. The baseline model χ2 was 17.2 (p<0.001), which included age, systolic BP and exercise capacity. With the addition of HbA1c, the model χ2 increased to 26.2 (p=0.003 for change from step 1). Finally, the addition of GLS to the model increased overall power (χ2=30.1; p=0.050 from previous step). Substitution of GLS by EF (multivariate HR=0.16 [0.00 to 10.40]; p=0.390) in a separate stepwise model did not yield statistical significance (p>0.05).
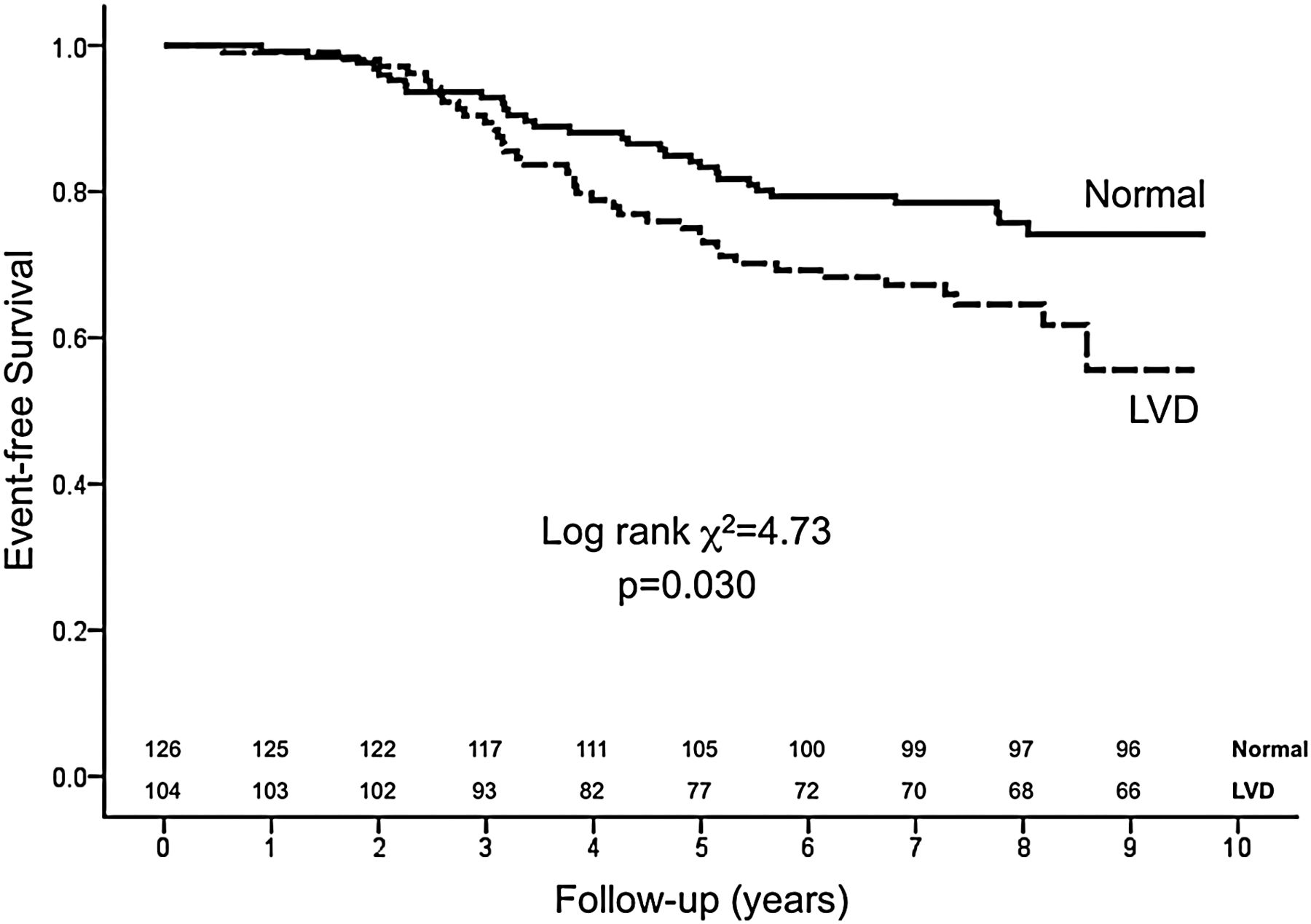
Kaplan–Meier survival curves were constructed for the primary endpoint, with log-rank testing for significance between strata. Those with LVD had significantly worse outcome than those without evidence of subclinical heart disease (χ2=4.73; p=0.030; figure 2).

{kind=link}
{kind=link}
Subclinical LV dysfunction (LVD) in type 2 diabetes and the risk of adverse outcome. Patients with evidence of LVD by global longitudinal strain had significantly worse outcome (primary outcome of all-cause mortality and hospitalisation) than those with normal strain. The number of subjects remaining in the analysis is displayed for patients with normal LV function and for those with subclinical LVD.
GLS was also associated with the secondary outcome of all-cause hospitalisation (HR=1.11 [1.01 to 1.22]; p=0.037), independent of age (HR=1.03 [1.00 to 1.06]; p=0.051), systolic BP (HR=1.02 [1.00 to 1.04]; p=0.047), exercise capacity (HR=0.90 [0.76 to 1.06]; p=0.193) and HbA1c (HR=1.31 [1.11 to 1.54]; p=0.001). The identification of LVD was also independently predictive of the secondary endpoint (HR=1.73 (1.03 to 2.93); p=0.040). When the stepwise Cox models were performed for the secondary endpoint, the addition of GLS imaging in the final step resulted in significant improvement in model power (p=0.046), over clinical and biochemical information, as did the identification of LVD by GLS imaging (i.e. in a separate model; p=0.045). The assumption of proportional hazards was met for all analyses reported.
Discussion
To our knowledge, this is the first study in patients with type 2 DM to demonstrate the adverse long-term prognosis associated with subclinical LVD measured by GLS. Increasing age, poor diabetic control and hypertension were other independent correlates of long-term outcome. The patients with type 2 DM recruited for this trial were asymptomatic, had no evidence of overt LVD and had negative exercise echocardiograms and/or coronary angiograms. Despite the cohort being largely overweight, over half (57%) exercised to 80% of predicted levels, 69% had acceptable levels of serum HbA1c (<8%) and 75% of patients had normal renal function.
Assessment of subclinical LV dysfunction
The role of 2D GLS in the evaluation of LV function is well supported by previous studies demonstrating the detection of subclinical LVD in patients with normal EF9–11 and deterioration in strain over time despite no change in EF.21 Although isolated diastolic dysfunction is also a common finding in individuals with type 2 DM, subtle systolic dysfunction detected by strain imaging may precede overt abnormalities of LV filling.15 These findings demonstrate the capacity of strain imaging to detect subtle myocardial dysfunction when EF and diastolic function are normal, as well as small changes in systolic function over time. In the current study, almost half of the cohort had evidence of LVD by GLS, despite a normal EF, and it was patients that had the worst prognosis. Prior work by our group has demonstrated the incremental prognostic information of GLS when added to clinical information and assessment of myocardial function by EF and wall motion scoring.5 GLS compares well to EF measured by echocardiography22 and MRI,23 is reproducible5 ,9 and is not angle-dependent, unlike tissue velocity strain techniques.23 Importantly, increasing evidence suggests that 2D strain is able to reliably detect myocardial fibrosis,16 and, although multiple definitions are currently used for LVD, this technique appears to provide the earliest indicator of myocardial dysfunction.15
Diabetic cardiomyopathy is a common finding in the community, with a reported prevalence of 1.1%, and is associated with high mortality and morbidity.24 However, few studies have reported prognostic outcomes associated with subclinical LVD. An important study by Kiencke et al12 highlighted the high prevalence of diabetic cardiomyopathy and propensity for functional deterioration in patients with DM and LVD or LV hypertrophy. Although there were no statistical differences between groups for individual outcomes, those with evidence of diabetic cardiomyopathy had lower combined event-free survival than those without. In a population-based study, From et al25 described the development of new-onset heart failure in patients with DM and evidence of diastolic dysfunction. Although the development of diastolic dysfunction may precede overt systolic dysfunction in patients with DM, increasing evidence suggests that subclinical systolic dysfunction detected by GLS imaging may be the first sign of LVD.15 In our study, GLS was used to identify patients with subclinical LVD, the finding of which was significantly associated with the primary endpoint of all-cause mortality and hospitalisation.
Pathogenesis of LVD in type 2 DM
In Rubler's landmark paper, patients with long-standing DM, glomerulosclerosis and heart failure of unknown origin had postmortem evidence of myocardial hypertrophy, fibrosis and microangiopathy.26 A number of factors contribute to LV hypertrophy and the perivascular/interstitial fibrosis characteristic of LVD, including glycaemic control and hyperinsulinaemia,27 activation of the renin–angiotensin system28 and myocardial substrate metabolism.29
The current study supports the association between poor glycaemic control and adverse outcome. In a recent meta-analysis of five major trials in DM, intensive glycaemic control resulted in a reduced non-fatal cardiovascular event despite no effect on all-cause mortality.30 Subjects recruited in these trials included a significant proportion of patients with existing coronary artery disease and heart failure, whereas the current study enrolled patients who were free of cardiovascular disease. As such, event rates presented in this study are lower, but in keeping with the prevalence of underlying cardiovascular disease and support the target of tight glycaemic control. The benefit of improved control on the temporal evolution of LVD remains unclear.
Limitations
There are a number of limitations to the current study, which was conducted in a relatively small, asymptomatic cohort of patients with type 2 DM, free of cardiovascular disease and gross myocardial dysfunction. First, we did not recall patients at the end of follow-up to assess the development of myocardial dysfunction in those free of LVD at recruitment. As such, this study can only describe prognostic risk associated with the finding of LVD, not the factors that contribute to its development over time. Second, all data on hospital admissions were coded according to the International Classification of Diseases criteria and obtained through a centralised state-wide data linkage service, but the usual limitations of administrative data should be remembered. For patients hospitalised with multiple conditions, the principal diagnosis recorded on admission was used. For example, comorbid heart failure associated with presentations of acute coronary syndrome and other pathologies may not have been identified as the principal diagnosis. There were insufficient deaths to perform a formal analysis of mortality alone. Finally, at the time of recruitment the recommendations for the routine use of ACE inhibition in patients with type 2 DM were only emerging, and the relatively low use of ACE inhibitors and β-blockers may be explained by this. For this reason, a formal analysis of their impact on outcomes could not be undertaken.
Conclusions
The presence of LVD in asymptomatic patients with type 2 DM is independently associated with adverse outcome over long-term follow-up. 2D GLS imaging identifies patients most at risk of adverse events. Tight diabetic control and management of cardiovascular risk factors (i.e. hypertension) remain important therapeutic targets for preventing poor outcomes related to diabetic heart disease. Future trials are required to determine whether earlier and more aggressive medical therapy is warranted in these individuals.
Key messages
What is already known on this subject?
Type 2 diabetes mellitus accelerates the development of cardiovascular diseases such as coronary artery disease and heart failure.
What might this study add?
Echocardiography is the mainstay for assessment of myocardial structure and function. 2D strain imaging is able to identify subclinical LV dysfunction even in asymptomatic patients with a normal LVEF.
How might this impact on clinical practice?
This long-term study demonstrates poor prognosis associated with subclinical LV dysfunction in asymptomatic patients with type 2 diabetes mellitus. Early identification of subclinical LV dysfunction by strain imaging may identify patients at increased risk earlier in the disease course, enabling earlier intervention. Further studies are required to examine potential interventions and therapeutic targets.
Acknowledgments
We would like to acknowledge the help and assistance of Julie Holliday, Sarah McLennan, Leanne Short and Diana del Pilar Valencia.
References
Footnotes
Contributors THM, JBP and TS contributed to the conception and design of the study. BAH and RL contributed to the collection, analysis and interpretation of the echocardiographic data. DJH, THM, BAH, MDH, JLH, ZYF, JBP and TS contributed to the analysis and interpretation of clinical data. DJH, THM and TS drafted the manuscript, and all authors contributed to revising it critically. All authors have read and had final approval of the manuscript.
Funding This work was supported by the National Health and Medical Research Council of Australia (grant: 993601) and the Private Practice Trust Fund, Princess Alexandra Hospital, Brisbane, Australia.
Competing interests None declared.
Ethics approval Metro South Hospital and Health Service Human Research Ethics Committee and the Ethics Committee of the University of Queensland, and complied with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All available baseline clinical and morbidity and mortality data from this study are included in this manuscript and available to all authors.