Article Text

Abstract
Background Elevated plasma glucose levels on admission (APG) are very common in patients with acute coronary syndrome (ACS) and can be the first indication of diabetes mellitus.
Objective To provide insight into the prevalence of previously undiagnosed diabetes and to compare different methods of diagnosing diabetes in patients with ACS.
Methods Patients with ACS with elevated APG who participated in the BIOMArCS 2 glucose trial underwent an oral glucose tolerance test (OGTT) prior to discharge. 130 patients were included who underwent metabolic assessment. Of these, 109 had an OGTT and 13 patients had pre-existing diabetes.
Results The OGTT results were categorised as (previously) undiagnosed diabetes in 35% of patients (fasting plasma glucose (FPG) ≥7.0 mmol/l or 2-h post-load glucose ≥11.1 mmol/l) and impaired glucose metabolism in 44% (FPG 6.1–6.9 mmol/l or post-load glucose 7.8–11.0 mmol/l), so only 21% had a normal glucose metabolism. Undiagnosed diabetes could not be adequately predicted with APG, FPG or HbA1c (area under the ROC curve 0.61, 0.75 and 0.72, respectively). Patients with abnormal glucose metabolism were significantly older, had higher admission HbA1c values, a higher Killip classification and more often had a prior stroke than patients with normal glucose metabolism.
Conclusion 79% of hyperglycaemic patients with ACS were found to have abnormal glucose metabolism. As APG, HbA1c and FPG had a low sensitivity to detect undiagnosed diabetes, an OGTT appears to be the best test to assess the presence of previously undiagnosed diabetes or impaired glucose metabolism in hyperglycaemic patients with ACS.
- OGTT
- diabetes
- myocardial infarction
- hyperglycaemia
- incidence
Statistics from Altmetric.com
Introduction
Elevated plasma glucose levels on admission (APG) are common in patients admitted with acute coronary syndromes (ACS) and are associated with a high incidence of adverse clinical outcomes, particularly compared with patients with normoglycaemic ACS.1–5 Nevertheless, hyperglycaemia remains unrecognised and untreated in a considerable portion of patients with ACS.6 This observation can partly be explained by the lack of convincing results of studies that have evaluated the clinical effectiveness of strategies aimed at early and strict plasma glucose regulation. It remains to be established whether hyperglycaemia is a marker or therapeutic target and which strategy would be best.7 8 Consequently, clinical treatment guidelines do not contain strong recommendations in this respect.9 Furthermore, clinicians may consider an elevated APG as a parameter of the temporary physical stress that is a natural part of—and caused by—the ACS which will normalise once the coronary event is adequately managed. It should be realised, however, that elevated APG can also be a sign of hitherto unrecognised diabetes mellitus. In this respect, the lack of knowledge of an elevated APG is of concern as the prevalence of undiagnosed diabetes will be underestimated.
Early recognition (and treatment) of diabetes in these high-risk patients may be prognostically important for two reasons. First, in the UK Prospective Diabetes Study early treatment limited microvascular complications.10 Second, besides new diabetes, impaired glucose metabolism which can be considered a pre-diabetic state is also detected. Early detection allows early measures such as lifestyle interventions or (off label) metformin therapy to prevent deterioration to full diabetes.11 Physicians in the cardiovascular field should therefore be aware of the various diagnostic tools to detect undiagnosed diabetes and its basic treatment modalities.
The European Society of Cardiology and the European Association for the Study of Diabetes (EASD) already advocate investigating glucose metabolism in patients without known diabetes but with established cardiovascular disease (CVD) through an oral glucose tolerance test (OGTT).12 However, a recent survey in the Netherlands showed that 76% of cardiologists do not routinely measure HbA1c prior to discharge in patients with ACS.6 With this in mind, it is unlikely that the more labour-intensive OGTT is standard care in daily cardiology practice.
The aim of this report is to identify the occurrence of previously undiagnosed diabetes in patients with ACS with hyperglycaemia at admission, to compare different diagnostic methods for diabetes in patients with ACS and to stress their importance.
Methods
Patients
The current analysis was part of the ‘BIOMarker study to identify the Acute risk of a Coronary Syndrome’ (BIOMArCS 2) glucose study carried out in the Medical Centre Alkmaar. Briefly, this study investigated the safety and effectiveness of intensive glucose regulation. It included patients with a clinical diagnosis of ACS and an APG of 7.8–16 mmol/l who were then randomised to intensive glucose regulation with intravenous insulin or expectative glucose management. Major exclusion criteria were the use of subcutaneous insulin (ie, insulin-dependent diabetes mellitus, IDDM), creatinine >220 mmol/l, left ventricular ejection fraction <30% and an expected transfer to another hospital within 48 h.13 The study was approved by the local ethics committee and all patients provided written informed consent.
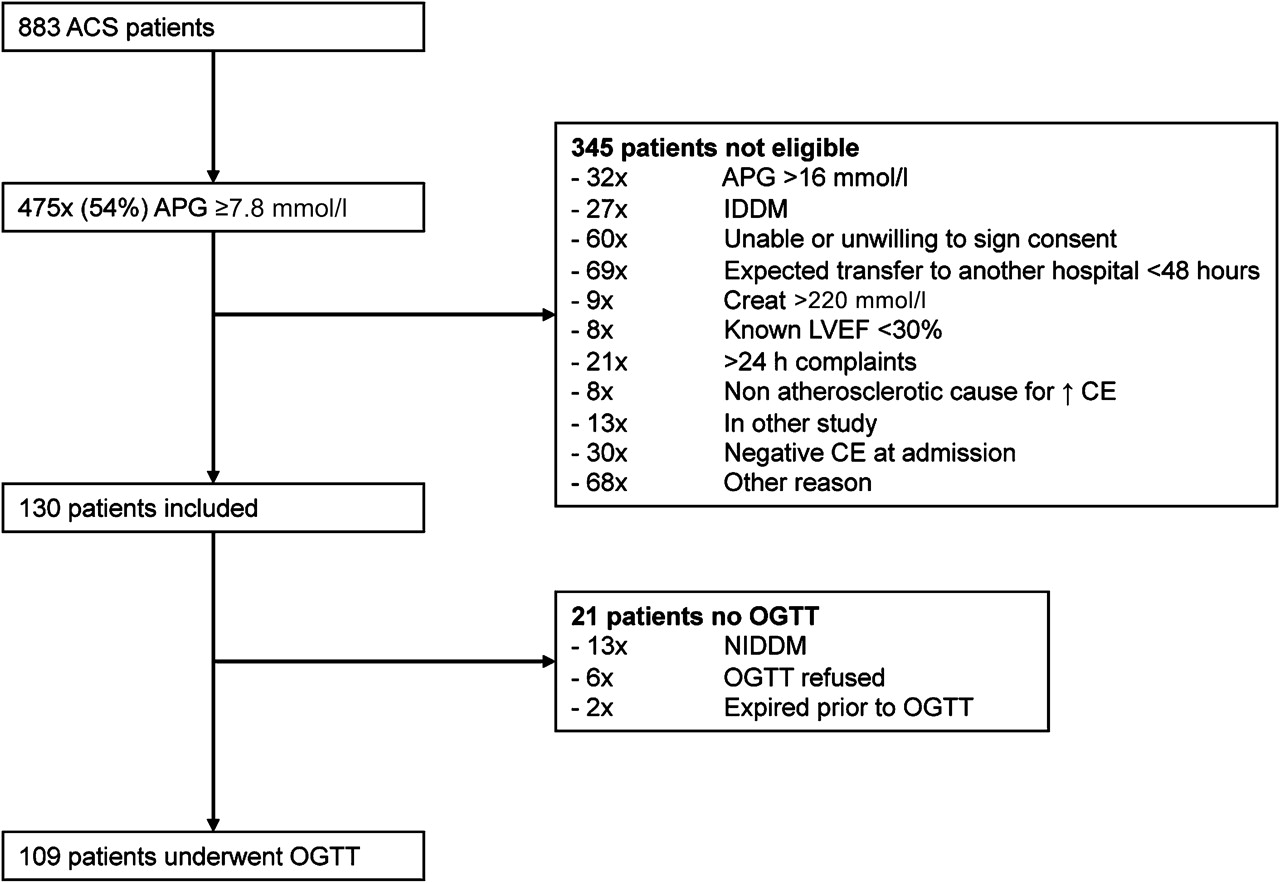
Between July 2008 and April 2010 a total of 883 consecutive patients with ACS were admitted; 475 patients (54%) presented with an APG of ≥7.8 mmol/l, 345 of whom met one or more exclusion criteria, and thus 130 patients were enrolled and form the study group. An OGTT was performed in 109 patients. The test was not performed in 13 patients with established non-IDDM, 6 patients who refused the test and 2 patients who died before the test could be performed (figure 1).

Patient selection. ACS, acute coronary syndrome; APG, admission plasma glucose; CE, cardiac enzymes; (N)IDDM, (non)-insulin-dependent diabetes mellitus; OGTT, oral glucose tolerance test. Patients with NIDDM were defined as those currently using oral antidiabetic therapy.
The diagnosis of ACS was based on the following criteria: typical ischaemic chest pain for at least 15 min and either ST elevation >1 mm in two consecutive leads and/or elevated markers of myocardial necrosis (ie, troponin I level >0.45 μg/l; Beckman Coulter, Brea, USA) within 24 h after the onset of chest pain.
OGTT and undiagnosed diabetes
The OGTT was performed according to a standardised protocol with 75 g glucose. The protocol specified that the test be performed prior to discharge, preferably on day 3 of admission. Hitherto undiagnosed diabetes was defined as a fasting plasma glucose (FPG) of ≥7.0 mmol/l or a plasma glucose value of ≥11.1 mmol/l 2 h after loading with 75 g glucose (post-load glucose (PLG)), according to the American Diabetes Association (ADA) and WHO recommendations.14 15 Both FPG and PLG values were measured by the Central Hospital laboratory in venous whole blood using sodium fluoride tubes. For safety reasons, a PLG was only obtained when the FPG was <7.0 mmol/l. Impaired glucose metabolism was defined as either impaired fasting glucose (FPG 6.1–6.9 mmol/l) or impaired glucose tolerance (PLG 7.8–11.0 mmol). Patients who did not fall into either of these groups were considered to have normal glucose metabolism.
Admission HbA1c, FPG and APG were compared with the OGTT result as the gold standard in order to compare different diagnostic methods for detecting diabetes mellitus according to the ADA guidelines.14 ROC curves and the area under the curve (AUC) were calculated for APG, HbA1c and FPG in order to investigate an appropriate cut-off to detect previously undiagnosed diabetes.
Statistical analysis
Categorical data are presented as numbers and proportions and continuous data are presented as median values and the IQR. Kolmogorov–Smirnov tests were performed and proved to be non-significant, indicating a normal distribution of cases within continuous variables. Differences in baseline characteristics in relation to OGTT results were evaluated by the Pearson χ2 test (dichotomous data) or the Kruskall–Wallis test (continuous data). Variables with a p value <0.05 were further investigated to detect which of the three OGTT groups were different from each other. For this, Mann–Whitney and Pearson χ2 tests were used as appropriate.
All statistical tests were two-sided and a p value <0.05 was considered statistically significant. The analyses were performed using SPSS Version 14.
Results
One hundred and nine non-diabetic patients with ACS entered the analysis and underwent an OGTT. The median age was 64 years (IQR 55–73), 81% were men and 98% were of Caucasian origin. Patients were discharged after a median of 3.6 days (IQR 2.4–4.7). The median APG was 9.2 mmol/l (IQR 8.3–10.4). ST elevation was present in 92 patients (84%), who had a median APG of 9.4 mmol/l (IQR 8.4–10.4) compared with 8.6 mmol/l (IQR 8.3–9.6) in patients presenting without ST elevation (p=0.061).
The median FPG was 5.9 mmol/l (IQR 5.5–6.3) and the median PLG was 9.1 mmol/l (IQR 7.4–11.6). Diabetes was newly diagnosed in 38 patients (35%), impaired glucose metabolism was found in 48 patients (44%) and only 23 patients (21%) had normal glucose metabolism (figure 2). The diagnosis of new diabetes was based on an FPG of ≥7 mmol/l in 14 patients and a PLG value of ≥11.1 mmol/l in 24 patients. The side effects of the OGTT were limited to mild nausea. Patients with undiagnosed diabetes were significantly older, had higher admission HbA1c values, had more often experienced a stroke and were in a clinically worse condition as expressed by a higher Killip class (table 1).

Results of oral glucose tolerance test (OGTT). Left panel: cumulative percentage of fasting OGTT results. Right panel: cumulative percentage of 2-h OGTT results. Reference lines represent cut-off values for either impaired glucose metabolism (6.1 and 7.8 mmol/l) or diabetes (7.0 and 11.1 mmol/l).
Baseline characteristics and results of patients who underwent an oral glucose tolerance test (OGTT)
With an FPG of ≥7.0 mmol/l as a diagnostic cut-off, 14 of the 38 patients with undiagnosed diabetes were recognised (table 2). With this cut-off value the sensitivity was 37% and specificity 100% (figure 3, left panel).
Comparison of diagnostic methods for diabetes

Sensitivity and specificity curves for fasting glucose (FPG, left panel), HbA1c (middle panel) and admission glucose (APG, right panel) compared with the oral glucose tolerance test (OGTT) as gold standard. Reference lines represent diagnostic cut-off values for diabetes as recommended by the American Diabetes Association (FPG, 7.0 mmol/l; HbA1c, 6.5%; APG, 11.1 mmol/l).
With HbA1c ≥6.5% (48 mmol/mol) as the diagnostic cut-off, only 11 (29%) of the 38 patients with undiagnosed diabetes were detected (table 2). In these 11 patients the OGTT confirmed undiagnosed diabetes. In our series the sensitivity to detect undiagnosed diabetes in patients with ACS with elevated APG at this HbA1c cut-off value was only 29%, with a specificity of 100% (figure 3, middle panel).
In patients with undiagnosed diabetes the APG varied between 8.0 mmol/l and 16.0 mmol/l. An APG cut-off value with reasonable sensitivity and specificity to predict undiagnosed diabetes could not be determined. The optimal cut-off value at the crossing of sensitivity and specificity curves was an APG value of 9.3 mmol/l; however, sensitivity and specificity were only 56%. When the diagnostic cut-off for a random glucose test in symptomatic patients was used instead (ie, ≥11.1 mmol/l), the sensitivity was 16% and specificity 89% (figure 3, right panel).
The area under the ROC curve was 0.61 for APG, 0.75 for FPG and 0.72 for HbA1c (figure 4). These tests therefore discriminate poorly between patients with a positive and negative OGTT.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curves comparing different diagnostic methods for diabetes. The oral glucose tolerance test (OGTT) result was used as the reference. The area under the curve was 0.61 for admission glucose, 0.75 for fasting glucose and 0.72 for HbA1c.
Discussion
One in three hyperglycaemic patients with ACS had previously undiagnosed diabetes and 44% were found to have impaired glucose metabolism. The strength of this study is the direct comparison of the four diagnostic methods for diabetes in these high-risk patients.
A pre-discharge OGTT was a more sensitive method for detecting undiagnosed diabetes and impaired glucose metabolism than APG, FPG and HbA1c. These results confirm the important role of an OGTT in detecting previously undiagnosed diabetes. They also show that diabetes is a common finding in hyperglycaemic patients with ACS, with or without ST elevation.
These results extend the current knowledge of the prevalence of undiagnosed diabetes in patients with myocardial infarction (MI) in the fibrinolysis era, in elective consultations for CVD and in patients who underwent an elective percutaneous coronary intervention, where the prevalence found with an OGTT was 31%, 22% and 16%, respectively,16–18 to the prevalence of undiagnosed diabetes in hyperglycaemic patients with ACS.
Diagnostic criteria to detect diabetes
Four criteria exist to diagnose diabetes: HbA1c, OGTT, fasting glucose and a random glucose test in a patient with classic symptoms of hyperglycaemia.14 Which of these is most appropriate for detecting undiagnosed diabetes in the setting of ACS remains to be clearly defined.
With HbA1c ≥6.5% (48 mmol/mol) as the diagnostic cut-off value, the AUC was 0.72 in our series, indicating that it is a suboptimal test to detect diabetes (figure 4). Compared with the OGTT, HbA1c missed 71% of patients with undiagnosed diabetes. In addition to 6.5% as the diagnostic cut-off for diabetes, the ADA recommends the use of a HbA1c value of 5.7–6.4% (39–46 mmol/mol) to identify patients with an increased risk of future diabetes.14 However, in this latter HbA1c group of 59 patients, the OGTT identified 31% of patients as currently having undiagnosed diabetes. There may be several reasons for the limited sensitivity of HbA1c to detect undiagnosed diabetes. As HbA1c correlates with the mean blood glucose over the previous 8–12 weeks, it requires regularly elevated glucose levels to increase. As a consequence, HbA1c levels rise above the diagnostic threshold at a later stage than direct glucose level measurement with an OGTT. Furthermore, in spite of standardisation, there are biological and patient-specific factors that can influence HbA1c results, such as haemoglobin variants, erythrocyte survival and turnover and race19–21 (see also http://www.ngsp.org). A ‘normal’ HbA1c value may therefore not be the most accurate method to rule out diabetes.
Measurement of FGP is another method frequently used by clinicians to screen for diabetes in patients with an elevated APG. However, the FPG of the OGTT recognised undiagnosed diabetes in only 37% of our series and the AUC was 0.75 (figure 4). Thus, FPG is insufficient and, in addition, a PLG should be determined (ie, a complete OGTT) to detect diabetes adequately.
In patients with classic hyperglycaemic symptoms a random glucose level of ≥11.1 mmol/l can be used to diagnose diabetes. Elevated glucose levels on admission in patients with ACS are often considered a stress response and, although not suitable to diagnose diabetes, it was felt that it may predict the outcome of an OGTT. In this series, however, a reasonably sensitive cut-off value could not be determined. Although the probability of finding diabetes with an OGTT increased with increasing APG levels, this high specificity could only be obtained at the cost of a low sensitivity (figure 3). APG was therefore not useful to predict diabetes. This is further illustrated by the AUC of only 0.61 when ≥11.1 mmol/l was used as a cut-off point (figure 4).
As with any test, the OGTT has limitations. The timing of the test may be important. It is conceivable that, in the days following an MI, although the glucose levels have normalised the underlying glucose metabolism has not yet fully recovered, resulting in a false positive test. This matter remains controversial. Some studies question the reproducibility of an OGTT as the disturbances were found to be transient,22–24 whereas others suggest that an OGTT in the early phase of MI is appropriate.16 25 A strong correlation between the 2-h blood glucose values at discharge and at 3 months was found, indicating that raised blood glucose values are not only related to stress induced by the ischaemic event.16
Possible clinical consequence of abnormal glucose metabolism
The early detection of diabetes in patients with CVD offers the chance to make early lifestyle interventions in this high-risk population. Apart from the question of whether or not a pre-discharge OGTT is the optimal timing to detect diabetes, Høfsten et al found that higher pre-discharge OGTT values were associated with increased mortality.26 Hence, it may be important to recognise all patients at risk and thus to use a test that detects as many patients with (pre)diabetes as possible. The European Society of Cardiology/EASD guidelines therefore recommend that an OGTT should be used to assess glucose metabolism in patients without known diabetes but with established CVD.12
With patient risk management we aim to eliminate—or favourably modify—risk factors. Unfortunately, many of these factors such as age cannot be influenced. It is therefore even more important to manage the factors we can influence, including newly diagnosed diabetes. Haffner et al showed that patients with diabetes without previous MI have as high a risk of MI as non-diabetic patients with previous MI.27 This has provided the rationale for treating cardiovascular risk factors in diabetic patients as aggressively as in non-diabetic patients with prior MI. Perhaps the opposite is also valid, and abnormal glucose metabolism in patients with MI should be treated as aggressively as in diabetic patients.
Limitations of the study
The number of patients included is relatively small and selected from patients who participated in a single-centre randomised clinical trial; the true prevalence of undiagnosed diabetes should be confirmed in a larger cohort of patients from multiple hospitals and countries that represent the broad spectrum of ACS. The proportion of diabetes and pre-diabetes in patients with an APG <7.8 mmol/l is particularly interesting as these patients were not eligible for the current study.
It would also be of interest to repeat the OGTT in all patients after 1 or 2 years to investigate which patients advanced from impaired glucose metabolism to diabetes and vice versa. This would help to determine whether a pre-discharge OGTT is the proper timing.
Conclusion
Our results underscore the fact that previously undiagnosed diabetes mellitus in patients with ACS with an elevated APG occurs frequently, and only 21% of patients had a normal glucose metabolism. APG, FPG and HbA1c underdiagnosed diabetes compared with an OGTT.
As the OGTT is a straightforward, non-invasive and affordable test that can be performed during clinical recovery, we would advocate that it should become standard care in all patients admitted with ACS, at least in those with an elevated APG. This will result in early recognition of diabetes and pre-diabetes and, subsequently, earlier lifestyle and medical interventions.
References
Footnotes
See Editorial, p 3
The sponsors were not involved in designing the study; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Funding Foreest Medical School Grant Number FIO 0610, Alkmaar, The Netherlands, The Netherlands Heart Institute/Interuniversitair Cardiologisch Instituut Nederland (ICIN).
Competing interests None.
Ethics approval This study was approved by the Medical Ethics Committee Noord Holland.
Provenance and peer review Not commissioned; externally peer reviewed.