Article Text

Abstract
Background: Several prospective studies have evaluated the association between body mass index (BMI) and cardiovascular mortality among patients with type 2 diabetes; however, the results are controversial.
Objective: To investigate the association of different BMI distributions with total and cardiovascular mortality among diabetic patients.
Methods: A total of 30 534 Ukrainian men and 58 909 women with type 2 diabetes from the nationwide population-based diabetes register were included in this study.
Results: During a mean follow-up of 2.7 years, 7804 deaths were recorded, of which 3320 were due to cardiovascular disease. After adjustment for age, smoking and alcohol drinking, the hazard ratios across the five BMI categories (<23, 23–24.9, 25–29.9 (reference group), 30–34.9 and ⩾35 kg/m2) among diabetic men were 1.57 (95% CI 1.42 to 1.74), 1.16 (1.05 to 1.28), 1.0, 1.01 (0.91 to 1.12) and 1.24 (1.02 to 1.50) for total mortality, and 1.67 (95% CI 1.42 to 1.95), 1.30 (1.12 to 1.51), 1.0, 1.13 (0.96 to 1.34) and 1.54 (1.16 to 2.05) for cardiovascular mortality, respectively. The respective hazard ratios among diabetic women were 1.34 (95% CI 1.22 to 1.47), 1.00 (0.91 to 1.10), 1.0, 1.04 (0.97 to 1.12) and 1.27 (1.14 to 1.41) for total mortality, and 1.36 (95% CI 1.18 to 1.57), 1.06 (0.92 to 1.21), 1.0, 1.12 (1.01 to 1.25) and 1.35 (1.15 to 1.59) for cardiovascular mortality. Additional adjustment for systolic blood pressure, total cholesterol, history of cardiovascular disease, diabetes treatments and duration of diabetes affected the results only slightly.
Conclusions: This study indicated a U-shaped association between BMI and total and cardiovascular mortality among diabetic men and women.
Statistics from Altmetric.com
Overweight and obesity are important public health problems in the world.1 2 Two in three adults in the United States are currently classified as overweight (body mass index (BMI) 25.0–29.9 kg/m2) or obese (BMI ⩾30 kg/m2).3 More than one-half of adults in most European and other developed countries are overweight or obese, and the prevalence of obesity is increasing rapidly in these countries, which is becoming a problem also in developing countries.2 Overweight and obesity are currently recognised as important risk factors for cardiovascular disease (CVD) in the general population,2 4–7 but the association between BMI and total mortality has shown various results in prospective studies, including a U-shaped or J-shaped association,5 8 9 a direct association10 11 or no association.12
Type 2 diabetes is one of the fastest growing public health problems in both developed and developing countries. It is estimated that the number of diabetic people in the world will double from 171 million in 2000 to 366 million in 2030.13 CVD accounts for more than 75% of total mortality among patients with type 2 diabetes.14 Although obesity is very common in patients with diabetes, only a few prospective studies have evaluated the association between obesity and CVD mortality, and the results are controversial. One population-based study in Finland proved that obesity was one of a number of risk factors for total and CVD mortality among diabetic patients,15 whereas other studies did not support this finding.16–20 Moreover, in one US study, diabetic patients with low BMI (<26 kg/m2) had higher all-cause mortality than patients with high BMI (26–30 kg/m2).19 Until now, there have been no data on the association of different BMI distributions (including low-normal weight, high-normal weight, overweight, class 1 obesity and extreme obesity) with the risk of total and CVD mortality among patients with type 2 diabetes in a large population-based cohort. The aim of this study was to evaluate the BMI-related risk of total and CVD mortality in a nationwide cohort of Ukrainian patients with type 2 diabetes.
SUBJECTS AND METHODS
Subjects
Patients with known type 2 diabetes from all 25 regions of Ukraine and the city of Kiev were entered into the population-based register “System of Diabetes Mellitus Care in Ukraine (SINADIAB)”. SINADIAB data have been used repeatedly for epidemiological studies.21–23 The study protocol was approved by the ethics committee of the Institute of Endocrinology and Metabolism, Kiev. In total, there are 40 225 800 adults from these regions. Data input was from 6 October 1997 to 3 February 2007, varying depending on the region, with the majority of data input after 14 November 2004. Data from patients who were present on the register up to 1 December 2006 were analysed and all patients had at least 1 month of follow-up. A total of 145 284 patients with type 2 diabetes were included in the SINADIAB data. Patients who were being treated with diet only (n = 45 413) or patients without any treatment information (n = 8940) were not included in the analysis because some of these patients might be receiving oral glucose-lowering drug (OGLD) treatment which was not indicated in the register. After the additional exclusion of patients with any incomplete data in the analyses (n = 1488), the final sample comprised 30 534 men and 58 909 women with type 2 diabetes who received insulin or OGLD treatment.
The completeness of data was evaluated according to the health statistics data on diabetic patients, which was published in 2005.24 Only the data on diabetic patients, who received insulin treatment, can be viewed as complete because insulin treatment in Ukraine is free of charge. OGLD treatment is not yet free for patients; however recently, a plan to develop free-of-charge treatments was approved by the government.24 Therefore, data on all insulin-treated patients and a significant proportion of OGLD-treated patients were entered into the register and analysed according to the information supplied by the primary care doctors. Before patients’ data were entered into the register, a diagnosis of diabetes was confirmed according to WHO (1985) or European Association for the Study of Diabetes (EASD)/International Diabetes Federation (IDF) (after year 1999) criteria, or according to a former clinical diagnosis resulting in the prescription of OGLD with or without insulin. Data on age, duration of diabetes, smoking habits (never or past, and current smoking), alcohol habits (yes or no), history of coronary heart disease (CHD) and stroke, diabetic treatment status, measurements of height, weight, blood pressure level, serum total cholesterol level and cause of death, in accordance with the International Classification of Diseases (ICD) codes, were collected or measured by primary care doctors. Height and weight were measured without shoes and with light clothing. The measurements of height were rounded to the nearest centimetre and weight to 100 g. The BMI was calculated by dividing weight in kilograms by the square of height in metres. In this study, we only included the patients with type 2 diabetes who were diagnosed at the age of ⩾40 years or were classified as type 2 diabetes by their primary care doctors.
Prospective follow-up
The study cohorts were followed up until the end of 2006 through computerised register linkage. Mortality data were obtained from primary care doctors: according to the rules the National Diabetes Mellitus Registry primary care doctors should give a death record that includes causes of death. The ICD 10th revisions were used for coding the causes of death. ICD codes I00 through I99 were classified as CVD deaths.
Statistical analyses
Differences in risk factors at different levels of BMI were tested using analysis of variance after adjustment for age (table 1). The Cox proportional hazards model was used to estimate the association between BMI and the risk of total and CVD mortality. BMI was evaluated in five categories (<23, 23–24.9, 25–29.9 (reference group), 30–34.9, ⩾35 kg/m2). The proportional hazards assumption in the Cox model was assessed with graphical methods, and with models including time-by-covariate interactions.25 In general, all proportionality assumptions were appropriate. Additionally, restricted cubic spline (RCS) with four knots was used in Cox models to test non-linear association of BMI as a continuous variable of mortality.20 26 The analyses were first carried out adjusting for age, and further also for smoking, alcohol consumption, systolic blood pressure, total cholesterol, history of CVD, diabetes treatments and duration of diabetes. All statistical analyses were performed with SPSS for Windows 15.0 or SAS software 9.10.
RESULTS
Table 1 presents the general characteristics of the study population at baseline. During the mean follow-up of 2.7 years, 7804 deaths were recorded, of which 3320 were due to CVD.
After adjustment for age, smoking, and alcohol consumption (multivariable model 1), the hazard ratios across the five BMI categories (<23, 23–24.9, 25–29.9, 30–34.9 and >35 kg/m2) among diabetic men were 1.57 (95% CI 1.42 to 1.74), 1.16 (95% CI 1.05 to 1.28), 1.0, 1.01 (95% CI 0.91 to 1.12) and 1.24 (95% CI 1.02 to 1.50) for total mortality, and 1.67 (95% CI 1.42 to 1.95), 1.30 (95% CI 1.12 to 1.51), 1.0, 1.13 (95% CI 0.96 to 1.34) and 1.54 (95% CI 1.16 to 2.05) for cardiovascular mortality, respectively (table 2). The respective hazard ratios among diabetic women were 1.34 (95% CI 1.22 to 1.47), 1.00 (95% CI 0.91 to 1.10), 1.0, 1.04 (95% CI 0.97 to 1.12) and 1.27 (95% CI 1.14 to 1.41) for total mortality, and 1.36 (95% CI 1.18 to 1.57), 1.06 (95% CI 0.92 to 1.21), 1.0, 1.12 (95% CI 1.01 to 1.25) and 1.35 (95% CI 1.15 to 1.59) for cardiovascular mortality. Adjustment for systolic blood pressure, total cholesterol, history of CVD, diabetes treatments and duration of diabetes affected the results only slightly.
The hazard ratio curves derived from spline regression models showed a U-shaped relation between BMI and the risk of total and cardiovascular mortality in both men and women (all p<0.001) after adjustment for age, smoking and alcohol consumption (fig 1). The nadirs of BMI were 27.10 kg/m2 for men and 27.14 kg/m2 for women, in whom the total death risks were the lowest.
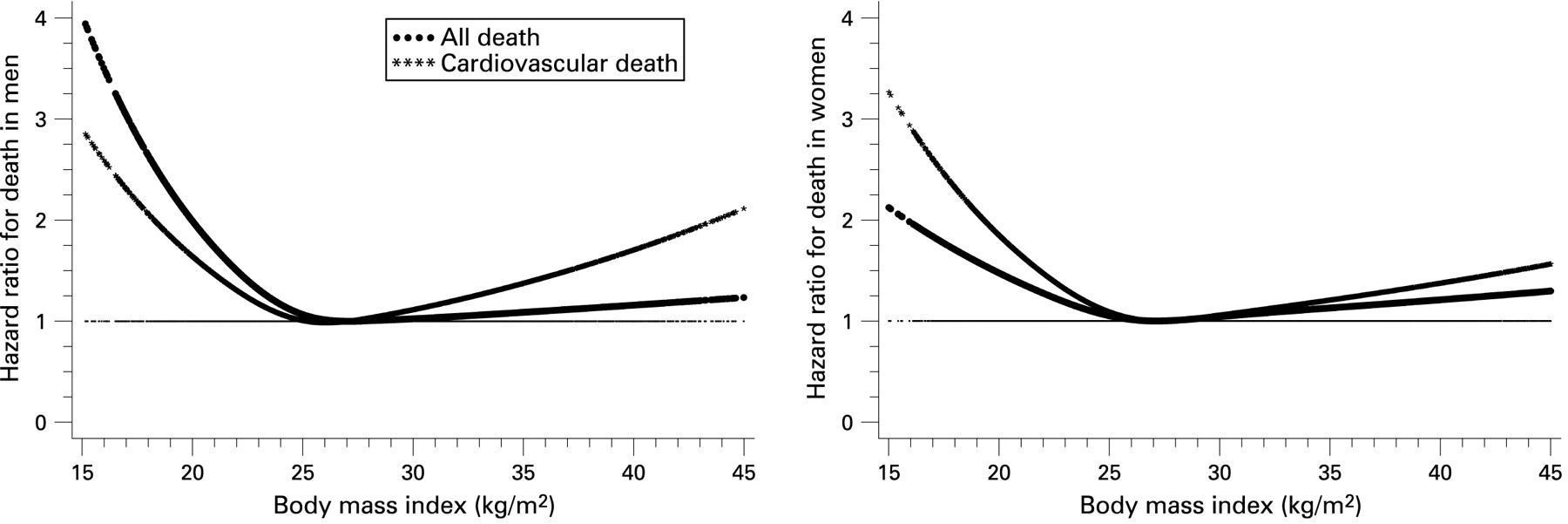
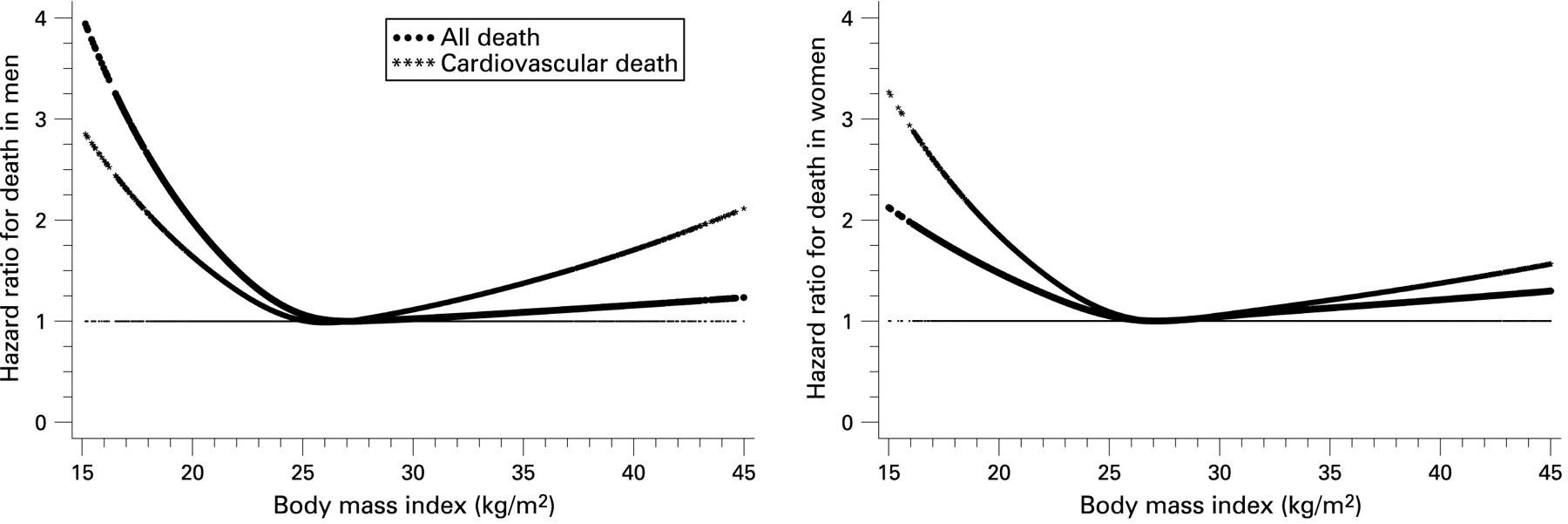{kind=link}
To avoid the potential bias resulting from severe diseases at baseline, additional analyses were carried out excluding the subjects who were diagnosed with CHD and stroke at baseline (n = 7840) (table 3). After excluding these patients, the hazard ratios of total and CVD mortality across the five BMI categories did not change. Exclusion of the subjects who died during the first 6 months did not affect the associations between BMI and the risk of mortality (data not shown).
In the analyses stratified by the smoking status, the U-shaped association of BMI on the risk of total and CVD mortality was seen in both non-smokers and smokers among men and in non-smokers among women (table 4). Similarly, the U-shaped association of BMI with the risk of total and CVD mortality was seen in diabetic patients with different types of treatment, and with short and long duration of diabetes.
DISCUSSION
In this population-based cohort study, we have indicated a U-shaped association between BMI and total and CVD mortality among men and women with type 2 diabetes. The risks of total and CVD mortality were increased in diabetic men and women with extreme obesity (BMI ⩾35 kg/m2), in diabetic men with low-normal (BMI <23 kg/m2) or high-normal weight (BMI 23–24.9 kg/m2), and in diabetic women with low-normal weight (BMI <23 kg/m2). Our results support one recent study in the general population from the National Health and Nutrition Examination Survey,27 which indicated that overweight was not associated with CVD and cancer mortality compared with normal weight.
Only a few prospective studies have evaluated the association between obesity and total and CVD mortality among diabetic patients, and the results are controversial. The results from the United Kingdom Prospective Diabetes Study indicated that high levels of BMI and waist-to-hip ratio were not major risk factors for CHD among diabetic patients,16 but this conclusion was based on only 79 cases of myocardial infarction in 2693 patients with type 2 diabetes. In the Veterans Exercise Testing Study, there was no association between BMI (as a continuous variable) and total mortality among 831 male veterans with diabetes.18 The direct association between BMI and total mortality among men with diabetes was found in the Aerobics Center Longitudinal Study; however, this association became non-significant when fitness was accounted for.17 One recent study from Finland found that diabetic patients with obesity, defined as the highest tertile of BMI, had a higher risk of total and CVD mortality than those in the lowest tertile of BMI, after controlling for many other potential risk factors.15 In the Pima Indian Community Study, there was a U-shaped association between BMI and total mortality among 814 subjects who were diabetic at baseline; however, an increased risk of total mortality was only seen among patients with low BMI (<25 kg/m2) and the highest BMI (⩾40 kg/m2) compared with patients with class I obesity (BMI 30–34.9 kg/m2).28 The results from the Hong Kong Diabetes Registry Study found a V-shaped association between BMI and total mortality among 7534 Chinese diabetic patients.20 Moreover, an increased risk of total mortality was found among Chinese diabetic patients with low BMI (<24 kg/m2) or high BMI (⩾27 kg/m2) compared with patients with median BMI (24–26.9 kg/m2).20 The results from the Translating Research Into Action for Diabetes (TRIAD) Study demonstrated an increased risk of total and CVD mortality among diabetic patients with low BMI (<26 kg/m2) compared with patients who were overweight (BMI 26–29.9 kg/m2).19 Unfortunately, there was no stratification of low-normal and high-normal weight in the TRIAD Study and the Pima Indian Community Study.19 28
This study is, to our knowledge, the first large prospective study to perform a quantitative evaluation of diabetic patients with low-normal and high-normal weight, overweight, class I obesity and extreme obesity on the risk of mortality. It is of note that most patients with type 2 diabetes are overweight: 15 365 men (50.3%) and 27 694 women (47.0%); and the mortality risk was the lowest in this group. This is the major reason why we chose overweight patients as the reference group in these analyses. Despite adjustment with numerous factors that may be linked to reversal causality during evaluation of mortality risks, the low-normal weight group (BMI <23 kg/m2) showed a higher relative risk of total and CVD mortality than the extreme obese group (BMI ⩾35 kg/m2). Possibly, patients with low-normal weight are associated with a clinical sign of insufficient insulin secretion. This could potentially lead to faster progression of nephropathy and, subsequently, increased mortality. Our preliminary analysis of death in this group showed a significant increase of end-stage renal disease, stroke and myocardial infarction (data not shown). We believe that patients with low-normal weight should be examined specially in order to expose any concurrent diseases (tuberculosis, malignant disease), in addition to the presence of diabetes with primary insulin secretion insufficiency, a subtype of type 2 diabetes. Patients with extreme obesity, defined as BMI ⩾35 kg/m2, should also be examined closely as there is significantly increased mortality among people in this group.
A review on guidelines for healthy weight by Willett et al1 identified three potential methodological problems that can distort the association between obesity and health outcomes. The most serious problem is reverse causation, another major concern is the adequate control for confounding factors and the third problem is the physiological effects of obesity, such as promoting hypertension, diabetes and dyslipidaemia. The two last concerns were statistically controlled for in our study. Also, we carried out sensitivity analyses excluding the subjects with a history of CHD or stroke at baseline and the subjects who died during the first 6 months. Exclusion of these events did not change our results.
In analyses stratified by the smoking status, a U-shaped association between BMI and total mortality was found among women who reported no current smoking and among men in all smoking categories. As expected, adjustment for obesity-related risk factors, such as blood pressure, lipids, diabetes treatments and duration of diabetes, weakened the association between BMI and mortality, but did not eliminate it. Our study showed an inverse association between BMI and current smoking status. The same relation was discovered by researchers from the Swedish National Diabetes Register.29 Obviously, diabetic smokers among men were associated with lower BMI, who had a greatly increased risk of mortality. It is necessary to consider such CVD-related confounding variables during evaluation of BMI-related mortality risks. However, consideration of smoking and alcohol use did not influence the significance of our results.
There are several strengths and limitations of our study. The sample size was large. A great number of CVD end point events were ascertained. We also excluded most subjects with type 1 diabetes from the analysis. A limitation of our study was that we did not have available information about physical activity and level of glucose control (diabetes severity). However, the fact that many patients were receiving insulin treatment might be considered as indirect evidence of a more severe course of diabetes. In this study, different types of treatment were considered as a confounding factor in the multivariable model and the association between BMI and mortality did not change in patients with either insulin or OGLD treatment. This is a primary care-based study of patients who entered into the local diabetes register. The studied cohort features a significantly higher proportion of women. Most probably, such a gender distribution exists across the whole Ukrainian population with type 2 diabetes. A recent cross-sectional analysis of an almost complete nationwide register of insulin-treated patients (105 364 patients ⩾30 years of age) showed a female preponderance in type 2 diabetic adults with insulin treatment in the Ukrainian diabetic population.30
In conclusion, this study demonstrates a U-shaped association between BMI and total and CVD mortality among men and women with type 2 diabetes. The risks of total and CVD mortality were increased in diabetic men and women with extreme obesity (BMI ⩾35 kg/m2), in diabetic men with low-normal (BMI <23 kg/m2) or high-normal weight (BMI 23–24.9 kg/m2) and in diabetic women with low-normal weight (BMI <23 kg/m2).
Acknowledgments
We are grateful to the Ukrainian primary care doctors who have included clinical data on their patients in the National Diabetes Mellitus Registry. Additional thanks for his constructive comments to Dr Nigel Harris (University of Bath, UK), coordinator of EU-funded medical informatics project (BSTD, PL 96–0121), participation in which accelerated the initiation of diabetes data recording in Ukraine.
REFERENCES
Footnotes
Funding: Grant support for this study was provided by the National Diabetes Mellitus Programme.
Competing interests: None.
Ethics approval: Approved by the ethics committee of the Institute of Endocrinology and Metabolism, Kiev.