Article Text

Abstract
Background Type 2 diabetes has been inconsistently associated with the risk of atrial fibrillation (AF) in previous studies that have frequently been beset by methodological challenges.
Design Prospective cohort study.
Setting The Atherosclerosis Risk in Communities (ARIC) study.
Participants Detailed medical histories were obtained from 13 025 participants. Individuals were categorised as having no diabetes, pre-diabetes or diabetes based on the 2010 American Diabetes Association criteria at study baseline (1990–2).
Main outcome measures Diagnoses of incident AF were obtained to the end of 2007. Associations between type 2 diabetes and markers of glucose homeostasis and the incidence of AF were estimated using Cox proportional hazards models after adjusting for possible confounders.
Results Type 2 diabetes was associated with a significant increase in the risk of AF (HR 1.35, 95% CI 1.14 to 1.60) after adjustment for confounders. There was no indication that individuals with pre-diabetes or those with undiagnosed diabetes were at increased risk of AF compared with those without diabetes. A positive linear association was observed between HbA1c and the risk of AF in those with and without diabetes (HR 1.13, 95% CI 1.07 to 1.20) and HR 1.05, 95% CI 0.96 to 1.15 per 1% point increase, respectively). There was no association between fasting glucose or insulin in those without diabetes, but a significant association with fasting glucose was found in those with the condition. The results were similar in white subjects and African-Americans.
Conclusions Diabetes, HbA1c level and poor glycaemic control are independently associated with an increased risk of AF, but the underlying mechanisms governing the relationship are unknown and warrant further investigation.
- Atrial fibrillation
- risk factors
- macrovascular disease
- smoking
- metabolic medicine
- epidemiology
- arrhythmias
- brugada
- QT interval
- heart rate variability
- sudden cardiac death
Statistics from Altmetric.com
- Atrial fibrillation
- risk factors
- macrovascular disease
- smoking
- metabolic medicine
- epidemiology
- arrhythmias
- brugada
- QT interval
- heart rate variability
- sudden cardiac death
Introduction
Atrial fibrillation (AF) is one of the most frequently sustained cardiac arrhythmias seen in clinical practice.1 Type 2 diabetes is a well-established risk factor for coronary heart disease (CHD) and stroke,2 and has been reported by some3–5 but not all6 observational studies to be associated with an increased risk of AF. The inconsistencies between study findings may in part be due to methodological challenges such as small sample size, limited adjustment for potential confounders, misclassification of exposure and using different methods of AF ascertainment. Furthermore, the relationships between common clinical markers of glucose homeostasis and incident AF have not been widely studied.
The Atherosclerosis Risk in Communities study (ARIC) provides an excellent opportunity to prospectively examine the association between diabetes and markers of glucose homeostasis with incident AF in a population of white subjects and African-Americans7 for whom there are no existing studies on this topic. The aims of this study were twofold: (1) to determine the risk of AF in individuals with diabetes compared with unaffected individuals; and (2) to investigate the relationships between levels of fasting serum glucose (FSG), fasting insulin and HbA1c levels with incident AF in individuals with and without diabetes.
Methods
The ARIC study is a community-based prospective cohort study of 15 792 participants aged 45–64 years at baseline and recruited from four communities in the USA.7 The first examination occurred in 1987–9, with three follow-up visits taking place, each 3 years apart. Participants (or proxy) are contacted annually by telephone to ascertain information on hospitalisations and deaths. Active community-wide surveillance of local hospitals was performed to identify additional hospitalisations. Visit 2 (1990–2) was the only visit for which stored whole blood samples were available for the measurement of HbA1c; this was the baseline for the present study unless otherwise stated. A total of 14 348 participants attended visit 2, of whom 1323 were excluded for the following reasons: non-white and non-African-American (n=91); prevalent AF or atrial flutter (n=114); no ECG or unreadable at baseline (n=273); non-fasting (<8 h) blood sample (n=471); missing information on exposure or covariates of interest (n=374). The final sample size was 13 025 individuals.
Blood collection and processing techniques from visit 2 have been previously described.8 Briefly, glucose was measured in serum using a hexokinase/glucose-6-phosphate dehydrogenase method. Insulin was measured by radioimmunoassay (125Insulin kit; Cambridge Medical Diagnosis, Bilerica, Massachusetts, USA) in visit 1 samples only.8 HbA1c was measured using high-performance liquid chromatography (Tosoh 2.2 Plus Glycohemoglobin Analyser in 2003–4 and the Tosoh G7 in 2007–8, Tosoh Corporation, Tokyo, Japan) on all participants with available stored whole blood at visit 2.9 The reliability of measurements from these stored samples has been previously reported.10
Attained educational level, income, cigarette smoking and use of antihypertensive and diabetic medications in the past 2 weeks were obtained from questionnaires and from documentation of medications.8 Sitting systolic BP was measured three times using a random zero sphygmomanometer after 5 min of rest. The mean of the last two measurements was used for the analysis. Body mass index (BMI) in kg/m2 was computed from weight in a scrub suit and standing height.
Study participants with FSG <100 mg/dl, HbA1c <5.7%, no use of diabetic medication and no history of physician-diagnosed diabetes were considered to have an optimal level of blood glucose and were categorised as having no diabetes.11 Individuals with FSG 100–125 mg/dl or HbA1c 5.7–6.4%, no use of diabetic medication and no history of physician-diagnosed diabetes were considered to have a suboptimal glucose profile and were classified as having pre-diabetes. Those with FSG ≥126 mg/dl or HbA1c ≥6.5%, use of diabetic medication or history of physician-diagnosed diabetes were categorised as having diabetes. Individuals with FSG ≥126 mg/dl or HbA1c ≥6.5% but no history of diabetic medication usage or physician-diagnosed diabetes were categorised as having undiagnosed diabetes.
Individuals with evidence of AF or atrial flutter on an ECG at visits 1 or 2 or a hospital admission for AF between the two visits were excluded from this analysis. Diagnoses of incident AF and atrial flutter were obtained to the end of 2007 from three sources: ECGs performed at study visits 3 and 4, presence of an ICD9 code for AF/atrial flutter (427.31 or 427.32) listed on the hospital discharge record, or AF listed as any cause of death on the death certificate. Hospitalisations with AF associated with open cardiac surgery were not considered events. The date of AF incidence was the earliest of any AF diagnosis. All ARIC examination ECGs were recorded using MAC PC Personal Cardiographs (Marquette Electronics, Milwaukee, Wisconsin, USA). A standard supine 12-lead resting ECG was recorded at each clinic visit and was transmitted by modem to the ARIC ECG Reading Centre for automatic reading and coding. All AF events automatically detected from the study ECGs were visually rechecked by a cardiologist.12
Analysis of data
Means (or percentages) and SDs were calculated separately in those with diabetes, pre-diabetes and those without diabetes. The age-standardised incidence of AF for both diabetes and pre-diabetes was calculated. Associations between diabetes and pre-diabetes with AF were estimated using time-dependent Cox proportional hazards models with time to AF as the dependent variable. Separate race and gender analyses were conducted; models were adjusted for age, study site, education, income, prevalent CHD, BMI, systolic BP, antihypertensive medications and smoking. Additional analyses included FSG in the model as a means to control for differences in control of diabetes. We explored the assumption of proportional hazards by computation of Schoenfeld residuals and inspection of log (−log (survival function)) curves.
Initially we explored the association between measures of diabetes markers and AF risk modelling FSG, fasting insulin and HbA1c using restricted cubic splines. After confirming linearity, the association between FSG, fasting insulin and HbA1c levels with incident AF was examined separately in diabetics and non-diabetics using Cox models with adjustment for the same covariates as previously described. χ2 Tests for trend were conducted across categorical levels and tests for interaction with gender and race were performed. p Values <0.05 were considered significant.
We conducted sensitivity analyses excluding individuals with a history of CHD prior to visit 2. Prevalent CHD included individuals with a history of myocardial infarction (MI), MI adjudicated from the baseline ECG or a history of coronary bypass or angioplasty. We also examined the associations between tertiles of FSG and HbA1c with incident AF after reclassifying individuals as diabetic or not diabetic based on a prior history of treatment for diabetes and self-reported history of diabetes (Y/N). To examine the relationship between duration of diabetes and risk of AF, self-reported age of diabetes diagnosis was obtained during an annual telephone follow-up between 1994 and 1996 among 10 371 individuals free of AF at visit 4 (1996–8).
Results
Baseline characteristics and prevalence of diabetes
At study baseline the mean age of the 13 025 participants included in this analysis was 57.0 years (table 1). One-third (33.7%) of the study population did not have diabetes, 51.4% had pre-diabetes and 14.9% had diabetes. Of those with diabetes, 50.6% were previously undiagnosed. During a mean follow-up of 14.5 years there were 1311 cases of incident AF. Of these, 98.9% were identified from hospitalisations, 6.6% from study ECGs and 5.6% from death certificates (some cases were identified by more than one method).
Descriptive statistics by type 2 diabetes status* at baseline (Atherosclerosis Risk in Communities study, 1990–2)
Incidence of atrial fibrillation by diabetic status
In the overall cohort, individuals with diabetes had an age-adjusted incidence rate of AF that was twice that of those without diabetes (9.02 vs 4.51 per 1000 person-years, p<0.0001). Those classified as having pre-diabetes had incidence rates of AF that were intermediate (5.14 per 1000 person-years). Compared with individuals who received a physician diagnosis of diabetes, those with undiagnosed diabetes had lower incidence rates of AF (10.8 vs 7.38 per 1000 person-years; p=0.0008).
Association between diabetic status and risk of atrial fibrillation
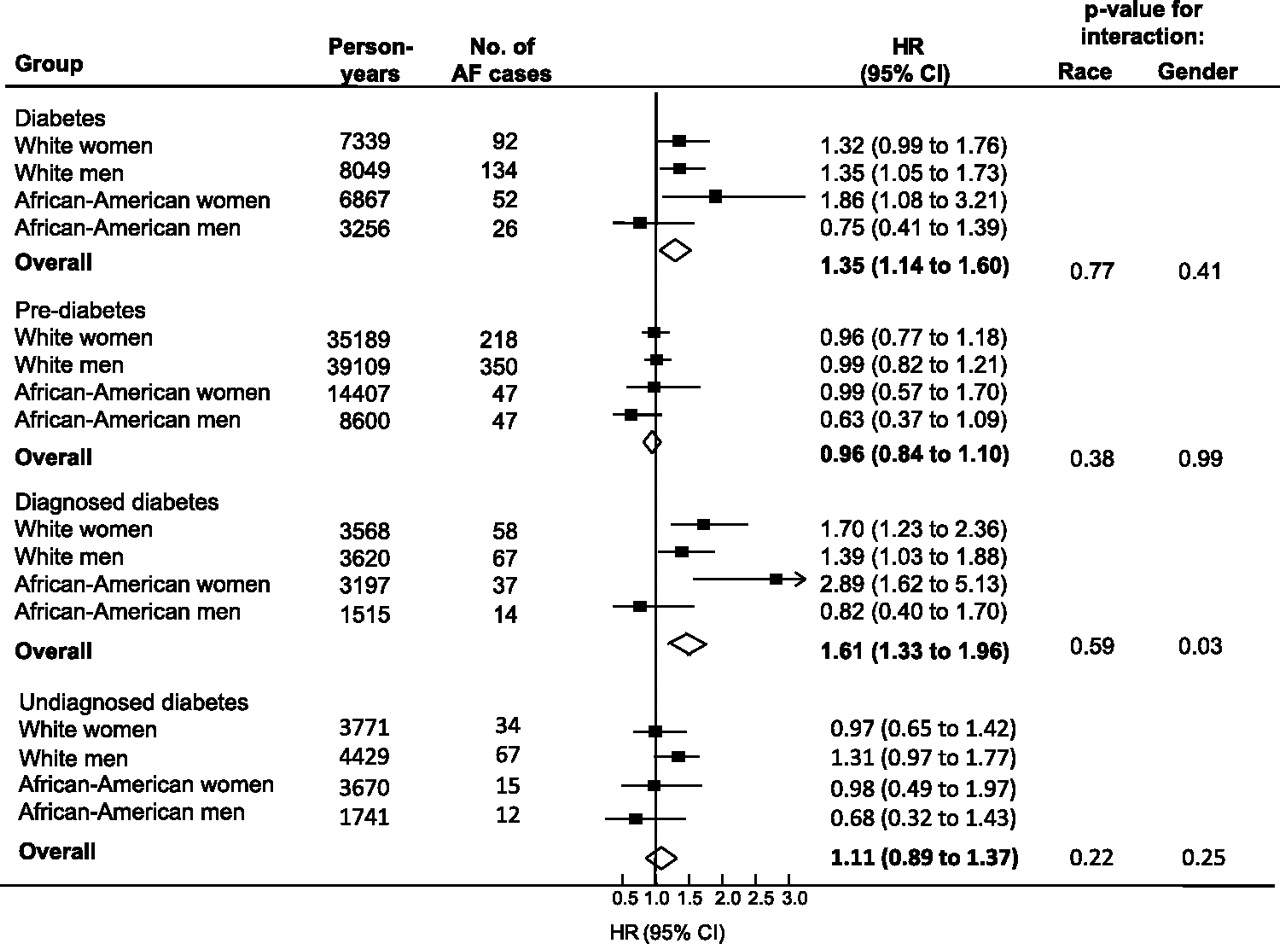
Individuals with diabetes had a one-third greater risk of incident AF compared with those without diabetes after adjustment with no evidence of interactions with race or gender (HR 1.35, 95% CI 1.14 to 1.60; figure 1). When FSG was included in the model to adjust for diabetes control, the risk of AF associated with diabetes was no longer significant (HR 1.07, 95% CI 0.87 to 1.33). After excluding those with prevalent CHD (n=12 307; 1150 cases of AF), the adjusted association between diabetes and risk of AF was attenuated (HR 1.27, 95% CI 1.06 to 1.52). After additional adjustment was made for FSG, the relationship was no longer significant (HR 1.04, 95% CI 0.83 to 1.31).
{kind=link}
Relationship between diabetes, pre-diabetes and physician-diagnosed diabetes with incident atrial fibrillation (AF) among white subjects and African-Americans in the Atherosclerosis Risk in Communities study by gender (1990–2007). Individuals without diabetes comprised the reference group for each comparison. Diabetes included all individuals with fasting serum glucose (FSG) ≥126 mg/dl, HbA1c >6.5%, use of diabetic medication or history of physician-diagnosed diabetes. Undiagnosed diabetes was defined as FSG ≥126 mg/dl or HbA1c >6.5% with no history of diabetic medication usage or physician-diagnosed diabetes. The black boxes represent the estimate of effect adjusted for age, education, income, prior history of cardiovascular disease, body mass index, systolic blood pressure, use of hypertensive medications and cigarette smoking. Horizontal lines represent the 95% CIs. Open diamond represents the estimate of effect for the overall population.
A positive association was observed in individuals with previously diagnosed diabetes but not in those with undiagnosed diabetes (HR 1.61, 95% CI 1.33 to 1.96 vs 1.11, 95% CI 0.89 to 1.37; figure 1). In individuals with diagnosed diabetes there was no interaction with race (p=0.59), but the association tended to be stronger in women than in men (p=0.03; figure 1). There was no evidence of an increased risk of AF in persons with pre-diabetes compared with those without diabetes after multivariable adjustment (HR 0.96, 95% CI 0.84 to 1.10) in any of the race or gender groups (all p values for interaction >0.35).
Association between fasting serum glucose and risk of atrial fibrillation
Among individuals without diabetes there was no evidence to suggest that FSG was independently associated with incident AF (p for trend=0.93), both overall or in any of the race/gender subgroups (all p values for interaction >0.30). Exclusion of those with prevalent CHD and undiagnosed diabetes did not materially alter these results (p for linear trend=0.13; both p values for interaction >0.13). Similarly, when diabetes was defined based only on history of medication use or self-report, there was no evidence of an independent positive association between tertiles of FSG and risk of AF among those without diabetes (p=0.63; table 2).
HRs (95% CIs) for atrial fibrillation (AF) by fasting serum glucose and HbA1c levels in individuals without type 2 diabetes (defined by no history of medication use or no self-report of diabetes; n=12 066) (Atherosclerosis Risk in Communities study, 1990–2007)
In individuals with diabetes there was a significant linear association between FSG and risk of AF (HR 1.03, 95% CI 1.01 to 1.05 per 10 mg/dl increase in FSG; p=0.0002), with no significant interaction by race (p=0.89) or gender (p=0.09). These results did not substantially change when individuals with undiagnosed diabetes were excluded (HR 1.03; p=0.002) or after further exclusion of those with prevalent CHD (HR 1.02; p=0.03). When diabetes was defined based only on history of medication use or self-report, there was similar evidence of a positive independent association across tertiles of FSG and AF (p=0.04; table 3).
HRs (95% CIs) for atrial fibrillation (AF) by fasting serum glucose and HbA1c levels in individuals with type 2 diabetes (defined by history of medication use or self-report of diabetes; n=959) (Atherosclerosis Risk in Communities study, 1990–2007)
Association between HbA1c and risk of atrial fibrillation
In individuals without diabetes there was a linear trend between incident AF and HbA1c level after adjusting for confounders (HR 1.05, 95% CI 0.96 to 1.15; p=0.07) for every 1% point increase in HbA1c. Exclusion of undiagnosed diabetics did not alter the results (HR 1.05), nor did the estimates differ by race (p=0.92) or gender (p=0.29). After excluding individuals with prevalent CHD (n=642; 131 cases of AF), the positive trend between HbA1c and incident AF was no longer apparent (HR 1.00, 95% CI 0.90 to 1.11). Similar results were observed when diabetes was defined on the basis of medication use or self-report (table 3).
In those with diabetes, HbA1c levels were positively and independently associated with incident AF (HR 1.13, 95% CI 1.07 to 1.20; p<0.001) per 1% point increase in HbA1c level. The result remained unchanged after excluding those with undiagnosed diabetes (HR 1.13; p=0.001) and those with prevalent CHD (HR 1.14; p<0.0001). Among all individuals with diabetes, after additionally adjusting for FSG, the relationship between HbA1c level and AF risk was attenauted (HR 1.11, 95% CI 0.99 to 1.24; p=0.07). Similar results were observed when diabetes was defined on the basis of medication use or self-report (table 3).
Association between fasting insulin and risk of atrial fibrillation
In an analysis based on 1530 AF events among 14 644 individuals, there was no evidence of an association across quartiles of fasting insulin and risk of incident AF in those with or without diabetes (both p for trends >0.50).
Association between duration of self-reported diabetes and risk of atrial fibrillation
Among 1541 persons with diagnosed diabetes at visit 4 with information on age at diagnosis, there were 179 incident cases of AF during follow-up beyond visit 4. There was an independent linear relationship between duration of self-reported diabetes and incident AF (p for trend=0.0006). Compared with unaffected individuals, those who reported having diabetes for <5 years had a 25% (95% CI 1% to 56%) greater risk of AF, and in those with diabetes for >10 years the risk was more than 50% higher (HR 1.58, 95% CI 1.17 to 2.13).
Discussion
Findings from this large community-based prospective cohort suggest that individuals with diagnosed diabetes, irrespective of race and gender, have a one-third greater risk of incident AF compared with individuals without diabetes, consistent with earlier studies.13 14 Furthermore, FSG was independently associated with a greater risk of AF in subjects with diabetes, an association which remained after excluding individuals with undiagnosed diabetes and prevalent CHD. This finding is consistent with a report from the US Cardiovascular Health Study which showed an independent positive association between FSG and AF in older adults in the USA.4
There was no evidence, however, to support the hypothesis that individuals with pre-diabetes are at increased risk of AF compared with those without diabetes. Similarly, in individuals without diabetes there was no association between FSG with AF, which is in agreement with findings from a Scottish cohort which reported no significant association between FSG and AF in healthy middle-aged participants.5
The current study does, however, support a positive and independent relationship between HbA1c levels and incident AF in individuals with and without diabetes. Moreover, our finding of a strong positive association between HbA1c level and the risk of AF in people with diabetes supports the hypothesis that poor glycaemic control is an independent risk factor for AF.
To the best of our knowledge, this is only the second report (and the first cohort study) to assess the association between HbA1c levels and risk of AF. In a previous case-control study a 1% point higher HbA1c level was associated with a 1.14 (95% CI 0.96 to 1.35) greater odds of AF15; however, as people with diabetes were included in that analysis, it is uncertain whether the association was due in part to a treatment effect. In the current study we surmounted this limitation by stratifying the analysis by diabetic status; in unaffected individuals a 1% point increase in HbA1c level was associated with a non-significant 5% greater risk of AF and a significant 13% greater risk in those with diabetes.
The lack of any association between markers of glucose homeostasis with incident AF in those without diabetes suggests that the relationship between diabetes and AF may be a function of the severity of diabetes and apparent only after long-term cumulative exposure to hyperglycaemia. This hypothesis is supported by our findings of a stronger association of diabetes with AF among persons with a longer duration of diabetes, consistent with an earlier report.15 Alternatively, the association between those with diagnosed diabetes and subsequent AF may be due to surveillance bias; as patients with diabetes have a greater likelihood of developing co-morbidities, they are more likely to have more contact with the healthcare system than those without a diagnosis of diabetes. Hence, increased surveillance of patients with diabetes for other medical conditions, including AF, may explain the stronger association with AF than in patients without diagnosed diabetes who are less likely to receive the same level of medical scrutiny.
The mechanisms by which diabetes may increase the risk of AF are largely unknown. Previous reports have shown that insulin resistance is associated with an increased risk of left ventricular hypertrophy which is itself a major risk factor for AF.16 Although we did not observe an association between fasting insulin and incident AF, we cannot preclude a possible causative role for insulin resistance in the aetiology of AF for three reasons: (1) we were limited by only having a single measure of insulin, the variability around which was high, and therefore any association may have been diluted; (2) a single measurement of insulin is a crude marker of insulin resistance; and (3) in a previous publication from ARIC, individuals with the metabolic syndrome (of which insulin resistance is a key component) had a significantly greater risk of AF compared with unaffected individuals.17
The main strengths of this study are its prospective study design, its long-term follow-up of more than 14 years and standardised detailed information on a large number of possible confounders. There are, however, some limitations. First, the lack of complete data on subtypes of AF may have different associations with diabetes, although there is no reported evidence of heterogeneity in the magnitude or direction of the positive association between diabetes and subtype of AF.15 Second, as discussed in a previous ARIC publication, as cases of AF were mainly ascertained through hospital discharge codes, this may have led to under-ascertainment of events that perhaps were not severe enough to warrant hospitalisation.18
In summary, individuals with diagnosed diabetes are at an increased risk of subsequent AF compared with those without the condition. The lack of clear evidence for an association between pre-diabetes, undiagnosed diabetes and several indices of glucose control suggests that the detrimental impact of diabetes on the risk of AF occurs only after prolonged exposure to diabetes.
Acknowledgments
The authors thank the staff and participants of the ARIC study for their important contributions. Aaron Folsom of the Division of Epidemiology and Community Health, University of Minnesota provided critical feedback on earlier versions of the manuscript.
References
Footnotes
Funding The Atherosclerosis Risk in Communities study is carried out as a collaborative study supported by National Heart, Lung, and Blood Institute contracts N01-HC-55015, N01-HC-55016, N01-HC-55018, N01-HC-55019, N01-HC-55020, N01-HC-55021, and N01-HC-55022. This work was additionally supported by the National Heart, Lung, and Blood Institute grant RC1HL099452 and American Heart Association grant 09SDG2280087.
Competing interests None.
Ethics approval The Atherosclerosis Risk in Communities study protocol was approved by the institutional review boards at each site and informed consent was obtained from all study participants.
Provenance and peer review Not commissioned; externally peer reviewed.