Article Text

Abstract
Hyperuricaemia is common in subjects with cardiovascular disease, but is not commonly considered a true risk factor. Recent studies suggest that uric acid is biologically active and can stimulate oxidative stress, endothelial dysfunction, inflammation and vasoconstriction. Epidemiological studies have found that uric acid can independently predict the development of hypertension, as well as stroke and heart failure. Experimentally raising uric acid in animals increases blood pressure, and pilot studies suggest that lowering uric acid in humans can reduce blood pressure in hypertensive individuals. Uric acid may also have emerging roles in the pathogenesis of kidney disease, metabolic syndrome and diabetes. More studies need to be performed on the pathophysiology and clinical consequences of hyperuricaemia in cardiovascular disease.
- Heart Failure
- Coronary Artery Disease
Statistics from Altmetric.com
Introduction
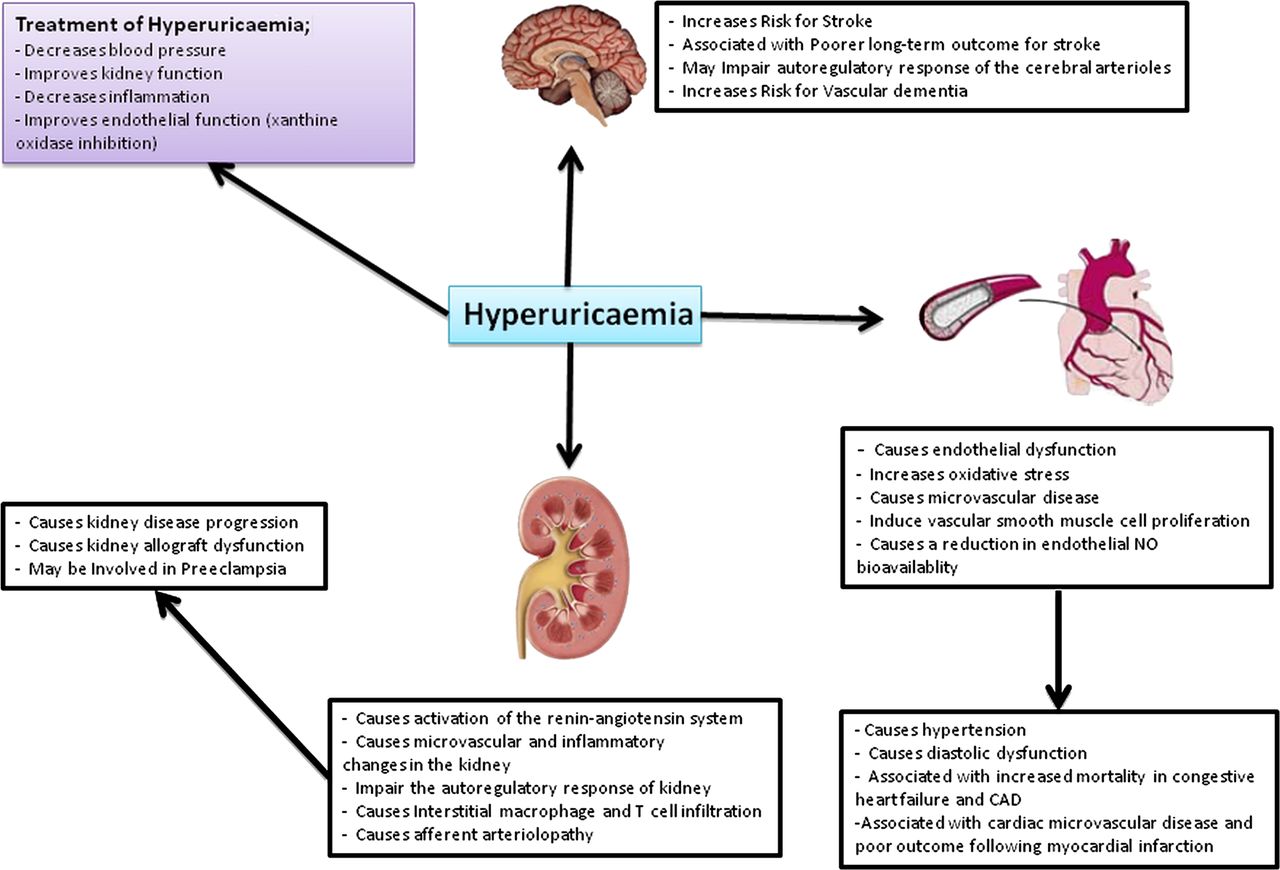
Uric acid is generated during the metabolism of nucleotides and adenosine triphosphate (ATP) and represents the end-product of purine metabolism in humans due to a mutation in uricase that occurred in human and ape ancestors nearly 15 million years ago.1 Although it was originally hypothesised that the loss of uricase activity carried evolutionary advantages by protecting against oxidative damage and prolonging life span owing to the antioxidant properties of uric acid,2 ,3 more recent studies suggest that the loss of uricase acted as a thrifty gene, which enhanced survival due to its ability to maintain blood pressure under low salt dietary conditions and to help enhance fat stores in the setting of food shortage.4 ,5 In the setting of native diets, the uricase mutation resulted in only a mild rise in serum uric acid to levels of 3–4 mg/dl range, similar to that observed among apes that also lack the uricase enzyme.6 ,7 However, with the introduction of Western diets rich in foods that can raise uric acid, such as fructose from added sugars, we have seen a dramatic rise in serum uric acid levels that has paralleled the marked increase in cardiovascular disease such as hypertension, stroke, coronary heart disease, renal failure, peripheral vascular disease, heart failure, obesity, metabolic syndrome and diabetes8 ,9 (figure 1). In this paper, we review the emerging evidence that uric acid may represent a true cardiovascular risk factor and some of the key countering arguments. A more extensive discussion can be found elsewhere.10

{kind=link}
Possible mechanisms by which uric acid might mediate cardiovascular disease, hypertension and kidney disease. CAD, coronary artery disease.
Uric acid and cardiovascular disease
Uric acid and hypertension
An association of elevated serum uric acid with the presence of hypertension was first noted in the 1870s and continued to be sporadically reported throughout the twentieth century. However, recent interest in uric acid as a true risk factor for hypertension has been generated by two major observations.
The first observation is that an elevated serum uric acid is a strong independent predictor of hypertension in almost every study published to date. In table 1, we summarised the prospective cohort studies with longer than 1 year of follow-up, with a sample size of at least 100 subjects, and regarding incident hypertension and uric acid.11–25 These observations are consistent with a meta-analysis including a total of 18 cohort studies representing data from 55 607 subjects which showed that hyperuricaemia was associated with an increased risk for incident hypertension (adjusted risk ratio=1.41; 95% CI 1.23 to 1.58). For 1 mg/dl increase in serum uric acid level, the pooled risk ratio for incident hypertension after adjusting for potential confounders was 1.13 (95% CI 1.06 to 1.20).26 Indeed, an elevated serum uric acid is the most reproducible independent risk factor for hypertension to date.
The prospective studies which explore the relationship between serum UA level and development of hypertension
The second major observation is that inhibition of uricase in the rat results in a rise in serum uric acid and development of systemic hypertension that is preventable by lowering uric acid with either xanthine oxidase inhibitors or uricosuric agents.27–29 The hypertension in this model was later shown to have two phases: an initial phase driven by the uric acid and mediated by endothelial dysfunction, oxidative stress and the activation of the renin angiotensin system, and a later phase driven by pathological microvascular and inflammatory changes in the kidney that was no longer dependent on uric acid levels.4 ,28 ,30 ,31 These two phases are similar to what is observed in human hypertension and for the progressive development of salt-sensitivity with age.32 ,33
Given the experimental studies, one might postulate that the lowering of uric acid would be most effective at lowering blood pressure in subjects who have not had hypertension long enough to develop subtle renal injury and inflammation. Indeed, the relationship of uric acid with hypertension is remarkably strong in adolescents presenting with hypertension.34 Consistent with this association, Feig investigated whether lowering uric acid with allopurinol lowers blood pressure in hyperuricaemic adolescents with newly diagnosed hypertension. They studied 30 adolescents (aged 11–17 years) who had newly diagnosed, never-treated stage 1 essential hypertension and serum uric acid levels ≥6 mg/dl. Treatment with allopurinol resulted in significant reductions of both clinical and ambulatory blood pressure.35 A similar reduction in blood pressure was also shown in prehypertensive adolescents with either allopurinol or probenecid (a uricosuric). Other studies have also demonstrated benefits on blood pressure in adults, although the effects are less dramatic.36 ,37 Clearly larger studies are needed before any definitive conclusions are drawn, but uric acid is emerging as a potentially modifiable risk factor for the prevention and treatment of hypertension.
Uric acid, heart failure and stroke
It is well known that the two major consequences of hypertension are stroke and heart failure, and numerous studies have shown a benefit of lowering blood pressure on these two conditions.38 If an elevated serum uric acid is a true risk factor for hypertension, then it readily explains why high uric acid levels also predict risk for stroke39–42 and heart failure.43 However, a complicating factor is that diuretics have been reported to be superior in the management of hypertension and heart failure compared with other commonly used antihypertensive agents,38 and thiazide diuretics have a side-effect of raising serum uric acid. This has led some authors to suggest that the rise in uric acid with diuretics might be beneficial, perhaps due to its antioxidant properties.44 However, many of the studies that used diuretics to show reductions in stroke and heart failure used chlorthalidone, which is particularly effective at lowering blood pressure throughout the 24-h period.45 ,46 Hence, the superior efficacy of chlorthalidone may not relate to its uric acid-raising effects, but rather to enhanced blood pressure control. Indeed, studies have suggested that the effect of antihypertensive agents on cardiovascular outcomes is worsened if the treatment raises uric acid levels (such as with diuretics)47 and improved if the agents lower uric acid (such as with losartan).48 Furthermore, in laboratory animals with metabolic syndrome, treatment with chlorthalidone resulted in a decrease in blood pressure with a rise in serum uric acid levels, but blood pressure was further improved if allopurinol was added.49
Uric acid might also increase the risk for stroke and heart failure by another mechanism, inducing microvascular disease. Years ago, Rao et al reported that uric acid can induce vascular smooth muscle cell proliferation,50 and later the mechanism was shown to involve the uptake of uric acid via specific transporters with the activation of Mitogen-activated protein (MAP) kinases and other mediator systems.28 ,51 ,52 The raising of serum uric acid has also been shown to cause arteriolar disease in the kidney and to impair the autoregulatory response.29 In turn, an impaired autoregulatory response of the cerebral arterioles is strongly associated with increased risk for stroke.53 ,54
The role of an elevated uric acid in subjects presenting with stroke is more controversial. While many studies suggest that an elevated serum uric acid is associated with poor long-term outcomes in subjects presenting with a stroke,55–57 there are also some studies suggesting that an increased uric acid might be associated with better short-term outcomes,58 an effect attributed to the antioxidant properties of uric acid.
In subjects with congestive heart failure (CHF), an elevated serum uric acid has been associated with reduced exercise capacity, inflammation markers, endothelial dysfunction, oxidative stress and diastolic dysfunction, and is predictive both of symptom status (ie, morbidity) and prognosis (ie, mortality).59 ,60 The risk for mortality with increasing serum uric acid levels is particularly striking, and increases markedly at serum levels of 7.0 mg/dl or higher.61–64 The source of the uric acid in these patients is likely multifactorial, and includes both increased generation from ischaemia-induced activation of xanthine oxidase in blood vessels and the coronary sinus,63 ,65 ,66 and increased uric acid reabsorption in the kidney from the effects of lactate on urinary urate transport.67 ,68
The strong association of serum uric acid with CHF severity and risk for mortality suggested the possibility that uric acid might have a role in the pathophysiology of CHF. It was postulated that this association may not be driven by the uric acid itself, but rather because xanthine oxidase generates oxidants during the production of uric acid.65 Consistent with these concepts, inhibition of xanthine oxidase with allopurinol was found to improve endothelial function in subjects with CHF,69 ,70 whereas there was no benefit when uric acid was lowered with the uricosuric agent, probenecid.71 In another study, the intracoronary administration of allopurinol in subjects with idiopathic dilated cardiomyopathy resulted in a significant decrease in myocardial oxygen consumption with no parallel decrease in stroke work, yielding a substantial improvement in myocardial efficiency.72 Inhibition of xanthine oxidase was also reported to reduce cardiac remodelling in laboratory rats with CHF.73
These observations led to a randomised study of subjects with moderate to severe CHF due to systolic dysfunction to receive either oxypurinol or placebo for 24 weeks. Using a composite end point for morbidity, mortality and quality of life, oxypurinol did not result in any clinical improvement. However, a post hoc analysis suggested that improvement was apparent in a subset of subjects with markedly elevated serum uric acid levels (>9.5 mg/dl) in which the degree of clinical improvement correlated with the degree of uric acid reduction.74 These data leave open the possibility that lowering uric acid with a xanthine oxidase inhibitor might be useful in some subjects with CHF and high uric acid levels.75
Uric acid and CAD
Whereas stroke and heart failure are closely linked with hypertension and arteriolosclerosis, coronary artery disease (CAD) is associated with additional risk factors for atherosclerosis such as hyperlipidaemia. Indeed, it has remained controversial as to whether uric acid is an independent predictor of CAD, with many studies favouring it as an independent risk factor48 ,76 ,77 and others coming to an opposite conclusion.78 ,79 Meta-analyses have not reached agreement as to the utility of uric acid as a cardiovascular risk factor.80 ,81 Table 2 summarises the prospective studies which have minimum 1 year duration of follow-up with a sample size of minimum 100 subjects regarding the studies between uric acid and coronary heart disease.39 ,80 ,82–87 Intervention studies would be helpful, but to date there has only been one randomised study of allopurinol in subjects with chronic stable angina, and while the results showed a benefit of allopurinol, the overall effects were modest and the study population small (n=65).88
Prospective studies regarding the UA and risk of coronary heart disease incidence
There is a common assumption with these epidemiological studies that uric acid is only causal in CAD if it is independent of other risk factors.89 However, if uric acid increases the risk for CAD as a consequence of causing hypertension then it would not be independent of hypertension as a risk factor. Thus, the best way to determine causality is to fall back on the principles of Koch, with experimental studies designed to evaluate cause and effect and with interventional studies in humans. At the base of these principles is an understanding of how uric acid might work at the cellular level.
Cellular actions of uric acid
Oxidant/antioxidant actions
Uric acid can react with a wide variety of oxidants, including singlet oxygen, peroxyl and hydroxyl radicals,3 ,90 ,91 and has been found to protect vascular endothelial cells from external oxidative stress.92 Unlike ascorbate, which can recycle after it is oxidised, the oxidation of uric acid results in its degradation to specific products. When uric acid reacts with superoxide, it generates allantoin, and this accounts for the increase in allantoin in the sera of patients who have CHF.69 Uric acid also reacts with peroxynitrite to generate triuret, and triuret levels are increased in subjects with preeclampsia.93 ,94 Uric acid can also react with nitric oxide (NO) directly, generating 6-aminouracil.95 ,96
The reaction of uric acid with peroxynitrite is not benign, but generates several radicals in the process, including the aminocarbonyl radical and the triuretcarbonyl radical,97 as well as intermediates with alkylating activity.93 Whether this is the mechanism remains unknown, but it is evident that the entry of uric acid into cells induces oxidative stress.98–101 Some studies suggest that the oxidative stress is associated with activation of nicotinamide adenine dinucleotide phosphate-oxidase (NADPH) and recent studies from our group suggest that oxidative stress is also occurring in the mitochondria.100 ,102 ,103 Rats made hyperuricaemic by a uricase inhibitor develop hypertension and evidence for oxidative stress, and the hypertension can be blocked by antioxidant treatment.30 Blocking oxidative stress also improves much of the proinflammatory effects of uric acid on vascular cells.98
Inflammation and vasoconstriction
It is well known that uric acid crystals can induce an inflammatory response, dating back to the 1960s when Faires and McCarty were able to reproduce symptoms of gout by injecting urate crystals into their own knees.104 However, more recent studies have shown that soluble uric acid can also activate inflammatory pathways resulting in the stimulation of chemokines (such as monocyte chemoattractant protein-1, MCP-1) and inflammatory markers (such as high sensitivity C reactive protein).52 ,105 The mechanism appears to involve uptake of uric acid into cells via organic anion transporters such as URAT-1, followed by induction of oxidative stress, the activation of specific mitogen activated protein kinases (including P38 and extracellular signal-regulated kinases (ERK)), and the nuclear transcription factors NFκB and APO-1.52 ,105 This leads to activation of vasoconstrictive mediators, including thromboxane, endothelin-1 and angiotensin II, as well as a release of growth factors including platelet-derived growth factor.4 ,52 ,98 ,102 ,106 Experimental studies suggest that uric acid-induced MCP-1 expression could be involved in animal models of hyperuricaemia,107 and similarly uric acid levels are associated with inflammatory markers in humans.108
Uric acid and endothelial dysfunction
While the antioxidant effects of uric acid can protect endothelial cells from external oxidative stress, most studies show that the entry of uric acid into cells is associated with a reduction in NO bioavailability via a variety of mechanisms, including by blocking uptake of L-arginine,109 stimulating L-arginine degradation via arginase,110 and by scavenging of NO from uric acid-generated oxidants100 or by uric acid itself.95 Endothelial dysfunction, as noted by a reduction in NO metabolites, has also been shown in the hyperuricaemic rat, and early supplementation of L-arginine can block the systemic hypertension and renal haemodynamic effects in this model.31 ,111 While uric acid has been reported to inhibit the NO-dependent dilation of isolated aortic rings in rats,112 this has not been universally observed.113 However, this may relate to where the aortic ring is derived, as the responsiveness of the aortic vascular smooth muscle cells to uric acid is dependent on the expression of URAT1 which is highly expressed in the abdominal aorta but not the thoracic aorta (W Chen, R Johnson and D Jala, unpublished). Importantly, hyperuricaemia is strongly associated with endothelial dysfunction in humans and lowering uric acid with xanthine oxidase inhibitors is strongly associated with improvement in endothelial function (table 3).36 ,69 ,70 ,71 ,114–123
Studies showing the relationship between reduction of uric acid and improvement in endothelial function
Uric acid and the renin angiotensin aldosterone system
As discussed earlier, uric acid has been found to stimulate angiotensin II in vascular endothelial cells98 and to also increase renin expression in experimental models.27 ,106 Experimental hyperuricaemia also stimulates aldosterone levels in the blood.124 Studies in humans have also found an association of plasma renin activity (PRA) and serum uric acid in patients with essential hypertension125 and PRA is higher in hyperuricaemic compared with normouricaemic children.126 Plasma uric acid level has also been reported to correlate positively with aldosterone excretion to the urine in healthy men.127 In a renal biopsy study, a correlation of uric acid with the percentage of renin positive juxtaglomerular cells was also found.128 Furthermore, Perlstein et al demonstrated that in a total of 249 subjects in high sodium balance, after adjusting for confounders, serum uric acid level independently and negatively predicted the renal plasma flow response to angiotensin II, consistent with evidence for increased intrarenal angiotensin activity in subjects with hyperuricaemia.129 Thus, there is increasing evidence for a relationship of uric acid with activation of the systemic and intrarenal renin angiotensin aldosterone system.
Innate immunity
Uric acid has also been found to be an important biological mediator released from injured, ischaemic or dying cells where it has a role in activating the innate immune system, involving both dendritic cells and CD8 positive T cells.130 ,131 The studies suggest that the activation is mediated by microcrystals of uric acid that is released by the dying cells. One of proteins associated with local inflammation132 is heat shock protein-70, and its induction can be blocked by allopurinol.133 The implication is that uric acid might have a role in the sterile inflammatory responses that occur in ischaemic tissues.
Other associations with uric acid
Because of space constraints, we do not review the strong associations of uric acid with the development of metabolic syndrome and diabetes, but there is increasing evidence that uric acid predicts the development of these conditions,134 and may have a contributory causal role.135 Uric acid, via its effects on inflammation, may also have a role in cancer.136
Major controversies with uric acid
While the data are compelling, there have been a variety of arguments that have weakened the uric acid hypothesis. One major argument relates to the antioxidant effects of uric acid. For example, the acute infusion of uric acid into humans is associated with improved endothelial function;137 ,138 these effects, however, might be expected since uric acid is being introduced initially into the extracellular circulatory system and the prooxidant effects require uric acid to enter the cells. Second, many authors have suggested that the benefit of xanthine oxidase inhibition is primarily via blocking the oxidants generated during the xanthine oxidase generation of uric acid. While this is likely one of the benefits of xanthine oxidase inhibition, reducing uric acid inside the cell may also be expected to reduce oxidative stress based on the numerous cell culture and animal studies.30 ,98 ,99 In addition, the observation that high dose allopurinol was more effective than probenecid in improving endothelial dysfunction in subjects with CHF71 might be expected, since allopurinol will block intracellular generation of uric acid in addition to lowering systemic blood levels. A third argument is based on genome-wide association studies. Specifically, several studies have shown that a composite of polymorphisms that are involved in regulating uric acid levels can be shown to predict gout but not cardiovascular disease.139 ,140 However, the primary polymorphism that was driving the uric acid levels was SLC2A9, which is a transporter that exports uric acid out of the cell. While gout is mediated by extracellular uric acid, the effects of uric acid on the cardiovascular system are mediated by intracellular uric acid levels, and hence one would not expect SLC2A9 polymorphisms that increase serum uric acid levels to predict cardiovascular disease.
Conclusions
In conclusion, there is increasing evidence that uric acid may have a key role in cardiovascular diseases, especially a role in hypertension and hypertension-related conditions. Uric acid may mediate these effects by inducing oxidative stress, inflammation, endothelial dysfunction and activation of the renin angiotensin aldosterone system. The data support the need for further investigation into the role of uric acid in cardiovascular disease especially since uric acid levels are effectively and safely modifiable with treatment.
References
Footnotes
-
Correction notice This article has been corrected since it was published Online First. Duk-Hee Kang's affiliation has been corrected to: “Division of Nephrology, Department of Internal Medicine, Ewha Womans University School of Medicine, Ewha Medical Research Center, Seoul, Korea”.
-
Statement The manuscript has been seen by all authors. It has not been submitted in similar form for publication elsewhere.
-
Contributors MK and BA generated the first draft of the manuscript that was carefully reviewed with additional contributions by RJJ, MS, DHK and BRI.
-
Competing interests RJJ has patent applications related to the lowering of uric acid and the blocking of fructose metabolism in the treatment of obesity and metabolic syndrome. He is also listed as an inventor on a patent by the University of Washington and Merck on the use of allopurinol to treat hypertension. RJJ also has two lay books entitled The Fat Switch (Mercola.com, 201) and The Sugar Fix (Rodale, 2008) that discuss the role of fructose and uric acid in the epidemics of obesity, diabetes and cardiovascular disease. RJJ has also consulted for several companies that are developing drugs for the treatment of hyperuricaemia, including Ardea, Biocryst and Novartis. All other authors list no conflicts.
-
Provenance and peer review Commissioned; externally peer reviewed.
-
Disclosures RJJ has several patent applications related to the lowering of uric acid as a means for preventing metabolic syndrome and hypertension.