Article Text

Abstract
Introduction Patients with diabetes in China have low health literacy, which likely leads to poor clinical outcomes. This study aimed to assess the effectiveness of health literacy and exercise interventions on clinical measurements in Chinese adults with type 2 diabetes mellitus (T2DM).
Research design and methods A cluster randomized controlled trial was conducted from February 2015 through April 2017 in Shanghai, China. 799 patients with T2DM aged 18 years or older recruited from eight Community Healthcare Centers were randomized into one control arm and three intervention arms receiving 1-year health literacy intervention, exercise intervention or both as the comprehensive intervention. Propensity score matching was employed to minimize potential imbalance in randomization. The intervention-attributable effects on main clinical outcomes were estimated using a difference-in-difference regression approach.
Results After propensity score matching, 634 patients were included in the analysis. The three intervention groups had decreased hemoglobin A1c (A1c) level after 12 months of intervention. The largest adjusted decrease was observed in the health literacy group (−0.95%, 95% CI: −1.30 to −0.59), followed by the exercise group (−0.81%, 95% CI: −1.17 to −0.45). However, A1c was observed to increase in the health literacy and the comprehensive groups from 12 to 24 months. No obvious changes were observed for other measurements including high-density and low-density lipoprotein cholesterols, and systolic and diastolic blood pressures.
Conclusions Health literacy and exercise-focused interventions improve glycemic control in Chinese patients with diabetes after 12 months of intervention, and the health literacy intervention shows the greatest effect. Our results suggest that the interventions may have the potential to improve diabetes self-management and reduce diabetes burden in China.
Trial registration number ISRCTN76130594.
- adult diabetes
- intervention trials
- health literacy
- exercise
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Previous studies have shown effectiveness of health literacy intervention and exercise intervention alone on type 2 diabetes mellitus (T2DM).
Good evidence exists for group-support and community-support self-management interventions in the prevention or delaying of diabetes complications, supporting the interventions among patients with diabetes in communities as a cost-effective approach.
Evidence on the effects of health literacy and exercise interventions on patients with diabetes in communities is yet to emerge.
What are the new findings?
Health literacy intervention and exercise intervention improve glycemic control in Chinese patients with T2DM, with a greater effect of health literacy intervention alone than the intervention with both components.
This cluster randomization trial, for the first time, provides evidence concerning the short-term and long-term effectiveness of the health literacy intervention, the exercise intervention as well as the comprehensive intervention (both health literacy and exercise interventions) for improving the clinical outcomes in patients with T2DM.
Both health literacy and exercise interventions were acceptable to participants and could achieve community coverage.
How might these results change the focus of research or clinical practice?
Implementation of interventions with a focus on health literacy and exercise has the potential for improving diabetes management and reducing diabetes burden in China.
Multi-interventions and mix-methods implementation research will be essential to better understand and develop population-level interventions that stimulate contextually specific actions to prevent and control T2DM.
Introduction
Diabetes is a chronic disease affecting approximately 425 million people worldwide in 2017,1 which imposes a large economic burden on individuals and families, healthcare systems and countries. In China, there are 114.4 million people with diabetes and the figure is estimated to increase to 119.8 million in 2045.1 People with diabetes, on average, have medical costs 2.3 times higher than those without the condition.2 With continuous increase in prevalence of diabetes, the health spending in treating the disease and preventing complications has increased from US$90 billion in 2015 to US$110 billion in 2017 in China.1
Due to the lifelong healthcare the condition entails, diabetes self-management is a major component of diabetes management.3 Adequate self-management requires patients to collect, process and comprehend diabetes-specific information in a manner that allows them to appropriately implement recommended treatment solutions related to diet and nutrition, exercise, weight and stress management and compliance with medication regimens.4 5 Specifically, exercise is considered a cornerstone of treatment for type 2 diabetes mellitus (T2DM) alongside diet and medication of proven efficacy.6 7 Despite the well-documented effectiveness of exercise in preventing or delaying diabetes and its complications,8 9 most people with T2DM are not active.10 The most common barriers include lack of knowledge, lack of motivation and misconceptions of physical activities.11
In China, although diabetes self-management strategy has been applied for years,12 13 only one-fifth of patients with diabetes were reported to achieve a hemoglobin A1c (A1c) <6.5%.14 One explanation is the low level of health literacy in Chinese patients with diabetes. Hu et al15 accessed diabetes-specific health literacy in Chinese rural patients with diabetes using the Questionnaire of Health Literacy of Diabetes Mellitus of the Public in China was designed by the Chinese Center for Health Education,16 and found that the average score was only 10.0, much less than the cut-off point of 19.5 defining the high or low health literacy level. The low health literacy and numeracy in Chinese patients greatly hindered the self-management implementation and effectiveness.17–19 Previous studies have shown associations between low health literacy and diabetes-related outcomes, including worse blood glucose control, misunderstanding of medication instructions20 and less knowledge about the disease.21 Studies also have demonstrated the significant role of health literacy in self-care, medication adherence and clinical outcomes.22 Thus, interventions should include strategies emphasizing on both health literacy and exercise to achieve optimal glycemic control and clinical outcomes, consequently. So far, however, little evidence is available on the effectiveness of intervention(s) with such components.
In our previous study based on a cluster randomized controlled trial (RCT), we reported a significant reduction in A1c in intervention groups.23 Due to the cluster randomization design, however, our results may be compromised by residual confounding effects due to incomparable baseline participant characteristics, although we have applied multivariable models to adjust for baseline covariates. To make baseline characteristics comparable at individual level, in this study we further assess the effect of health literacy intervention, exercise intervention as well as comprehensive intervention (including both health literacy and exercise) in patients with T2DM in China using a propensity score-matched approach (PSM).
PSM is a method that effectively balances the distribution of covariates between groups, ensuring further evaluation of the treatment effect close to that based on an RCT. PSM has advantages in selecting samples that could maintain baseline balance, and plays a significant role in promoting the design of cluster RCTs.
Methods
Study design and participants
The cluster RCT was conducted in 8 of a total of 26 community healthcare centers in Minhang and Changning districts of Shanghai, China.23 Three to five clinic sites were selected from each center. All clinic sites met the following criteria: (1) at least 20 patients can be recruited; (2) at least two to four physician(s), nurse practitioner(s) or diabetes educator(s) can participate in the intervention as a general practitioner (GP) team; (3) agrees to participate for a 100 patients with T2DM were recruited from each community healthcare center through the Diabetes Management system in Minhang and Changning Districts24 25 during the period of February 2015 and March 2016. After excluding one patient without measured baseline A1c, a total of 799 patients with diabetes were recruited from 35 clinic sites in eight community healthcare centers (as shown in figure 1). Inclusion criteria at the patient level included: (i) clinically diagnosed with T2DM according to the 1999 criteria of WHO; (ii) age 18–85 years; (iii) most recent A1c ≥7.5% (or fasting glucose ≥10 mmol/L); (iv) signed informed consent form by the patient and (v) patient’s agreement on 2-year participation in the study. Exclusion criteria at the patient level included: (i) poor visual acuity (vision worse than 0.1/4.0 using the Standard Logarithmic Visual Acuity Chart); (ii) significant dementia or psychosis (identified through health provider report or chart review); (iii) terminal illness with anticipated life expectancy <2 years and (iv) no permission from their physicians. Informed consent was collected from each participant.
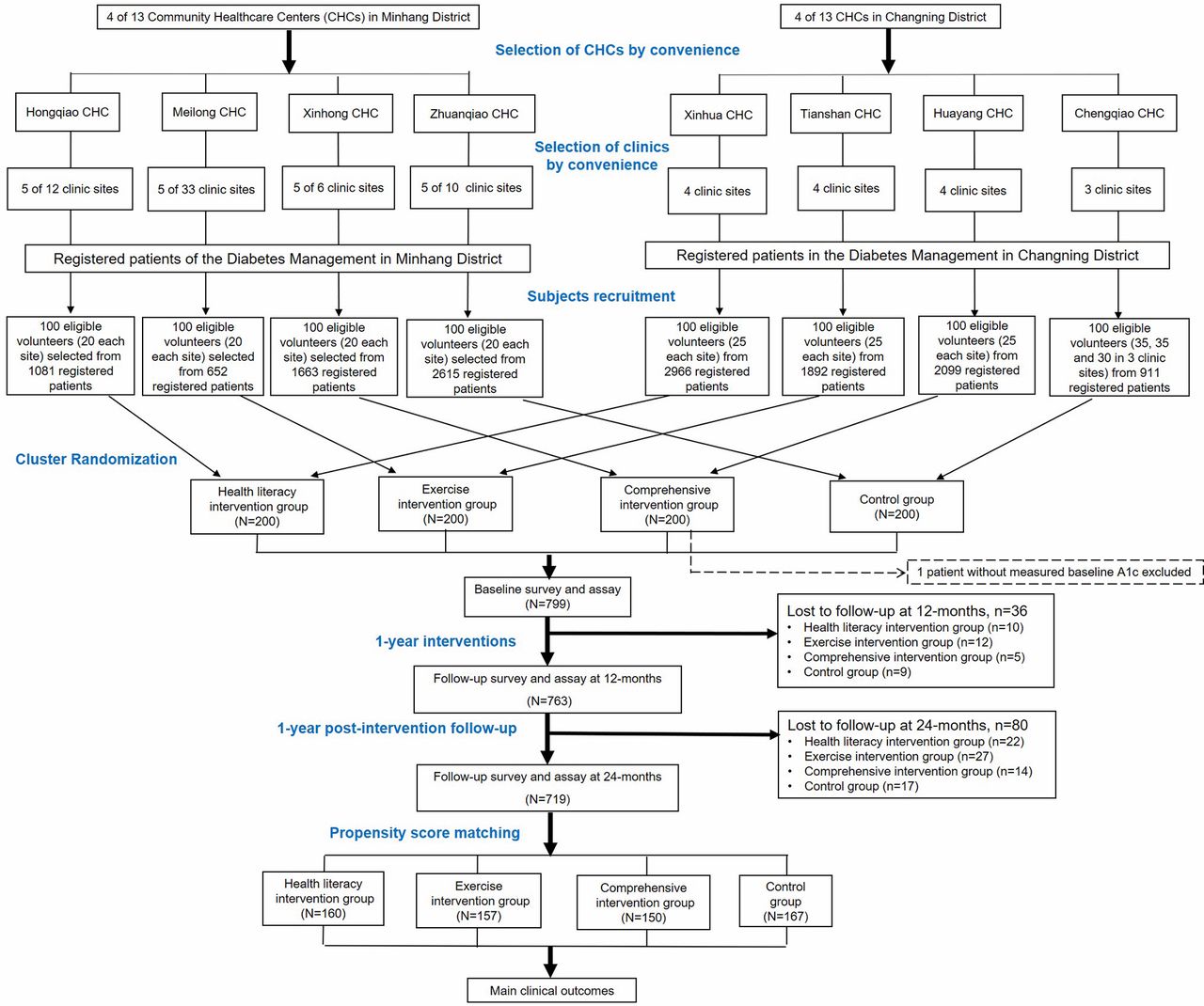
Flow chart of the study.
Randomizations
Randomization occurred at the community healthcare center level. Six community healthcare centers were randomized to receive interventions (intervention groups), whereby two centers (including nine clinics) received health literacy intervention, two (including nine clinics) received exercise intervention and two (including nine clinics) received comprehensive intervention with both health literacy and exercise components from baseline to 12 months, and all the three intervention groups received usual care from 12 to 24 months. Two centers (including eight clinics) were randomized to retain receiving usual care (control group) in 2-year study period. As a result, of 799 eligible participants recruited from 35 clinics in 8 centers (ie, clusters) via the GP teams, 200 were in the control group, 199 in the comprehensive group, 200 in the health literacy group and 200 in the exercise group.
Interventions
The control group in the 2-year study period and the three intervention groups in the second year received usual care for diabetes according to the Chinese National Guidelines. This included conventional clinical consultations, and treatment provided based on existing knowledge and at the individual clinician’s discretion. Neither specific training on communication skills, nor literacy-numeracy-sensitive Diabetes Education Toolkit materials were provided to the providers in the two control centers.
The health literacy-oriented intervention had two main components: the Partnership to Improve Diabetes Education Toolkit (PRIDE) and a Clear Health Communication Curriculum. The PRIDE toolkit was built based on a Toolkit developed and validated previously.26 It consists of 24 educational modules covering all components of diabetes self-management including diet, exercise, foot care, glucose monitoring, medication management and enhanced diabetes log sheets (online supplementary table 1). And the modules were written at a low literacy and numeracy level and designed specifically to improve patients’ understanding and self-management behaviors in those with poor literacy and/or numeracy skills. For example, the module of diet includes information on (1) nutrition for diabetes; (2) using your plate to control your carbs; (3) counting your carb grams; (4) What can I Eat for a Snack? and (5) What Should I Eat When I Eat Out? GPs from the centers in the intervention groups were trained to properly use the PRIDE toolkit and required to employ the materials during regular patient visits usually occurred every 2 weeks. At each visit, GPs covered at least two components from the toolkit materials, and performed and documented at least one goal-setting task with the patient. The GPs spent approximately 5–7 min per visit to share components of the toolkit directly with the patients. Nurses or health educators phoned the subjects to supervise. A structured training program was also employed among these healthcare providers in order to improve diabetes-related counseling communication skills, with the attention on issues of literacy and numeracy.
Supplemental material
Patients in the exercise group received usual diabetes care and were advised to walk 3–5 times a week, 30–40 min per time in the first 6 months and 60–70 min per time in the following 6 months. The intensity of exercise was ideally kept between 12 and 15 in the Borg Rating of Perceived Exertion visual scale. Each patient in this group was required to record the time and intensity of each walk on a calendar book which was checked by his/her GP team members. Patients in the comprehensive intervention group received both the literacy and exercise interventions.
Data collection
Information on health literacy level, numeracy skill and exercise level was collected using the Chinese versions of the Health Literacy Management Scale (HeLMS)27 and the Diabetes Numeracy Test (C-DNT-5),28 and the Global Physical Activity Questionnaire (GPAQ), respectively. Demographic characteristics, diagnosis of diabetes, duration of diabetes, smoking status, dietary habits (measured by 3 days 24 hours dietary recall), physical activities (evaluated using the GPAQ) and use of antidiabetes drugs were collected at the baseline survey. Body measurements and biochemistry assays of A1c, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), systolic blood pressure (SBP) and diastolic blood pressure (DBP) were performed and the information was recorded at each survey, that is, baseline, 12 months (post-intervention) and 24 months (1-year post-intervention).
Statistical analyses
All analyses were conducted using Stata V.12.0 software. The effects of interventions were assessed at the end of intervention by comparing levels of major clinical measurements such as A1c, HDL-C, LDL-C, SBP and DBP at 12 months with those at baseline, and the long-term sustainability of the effect were evaluated at the end of 1-year post-intervention by comparing levels of major clinical measurements at 24 months with those at 12 months.
Given no randomization was performed at the patient level due to the study design, we employed PSM among participants to minimize any potential imbalance between groups at baseline. Propensity scores were calculated based on logistic regression. Baseline characteristics were included as independent variables, with those statistically significant (p<0.05) and/or considered potential confounders retained in the final model. Eventually, the final model included age, sex, education, household income per month, diabetes duration, A1c level, HeLMS score, C-DNT-5 score and metabolic equivalent of physical activities; 1:4 neighbor with replacement radius matching method was used with a radius of 0.25 in the base case scenario.
Multiple linear regression models were used to compare the main clinical outcomes in three intervention groups and their matched control groups at baseline, 12 months and 24 months. In order to estimate the intervention-attributable effect on main clinical outcome, difference-in difference (DID) regression approach was also employed, defined as below:
where yij is the main clinical outcome level by the ith participant in the jth survey, Gij indicates the intervention, Tij indicates the survey time, the interaction term Gij×Tij indicates the difference in the intervention and control groups during the intervention time, Xkij represents the potential confounder k, and β0 and εij represent the intercept and error term in the model, respectively. The difference in the between-round changes in the quality scores for each megacity yielded an estimate of β3. Gij represent intervention or control group, Tij represent before or after interventions. We also adjusted potential confounders, such as age, sex, education, household income per month, diabetic duration, smoking status, antidiabetic drug use and insulin use in the DID regression. We ran models for each clinical measurement including A1c, HDL-C, LDL-C, SBP and DBP. Therefore, in the DID regression model, β1 represent the effect of clustering, β2 represent time effect and β3 represent the intervention-attributable effect.
In order to test the robustness of the results, the full sample before PSM and the sample after neighbor and radius propensity score matching technique were used for sensitivity analysis. Regarding the neighbor and radius propensity score matching technique in the sensitivity analysis, a 1:1 neighbor with replacement radius matching using a radius of 0.05 was performed. The SD of propensity score after a 1:1 neighbor is 0.2. According to the principles of PSM, the radius can be calculated by the SD multiplied by 0.25, which is 0.05. This means that we matched 1:1 observation of a 5% difference in propensity scores. In addition, the DID analysis was performed to check the robustness of the model.
Role of the funding source
The funder of the study had no role in study design, data collection, data analysis, data interpretation or writing the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Results
A total of 799 patients with T2DM completed the baseline survey. During the 2-year period, 36 patients were lost during the baseline to 12 months follow-up period, and 80 were lost during 12–24 months follow-up period. After matching, 634 patients consisting of 167 in the control group, 150 in the comprehensive intervention group, 160 in the health literacy group and 157 in the exercise group were included in the analysis (figure 1).
Table 1 shows the baseline information of the subjects before and after PSM. Before PSM, the subjects in the health literacy, the exercise, the comprehensive and the control groups were comparable in age, sex, duration of diabetes, body mass index and A1c level, but were significantly different in education, income, occupation, glucose-lowering drugs and insulin use and health literacy level (p<0.05). After PSM, no significant differences were observed for these characteristic factors between any intervention group and the control group (all p values >0.05).
Baseline demographic characteristics of subjects before and after propensity score matching (PSM)
In the literacy group, DID analysis showed that literacy intervention attributed an improvement in glycemic control at 12 months compared with that at baseline, with A1c decreasing by 0.95% (95% CI: −1.30 to −0.59) during the period. However, 0.33% (95% CI: 0.04 to 0.63) increase in A1c was observed in the group at 24 months compared with 12 months (table 2). For other clinical measurements, an increase in LDL-C (0.67 mmol/L, 95% CI: 0.41 to 0.93) and in DBP (2.03 mm Hg, 95% CI: 0.08 to 3.99) was observed during the 1-year intervention period, whereas a decrease in SBP (−1.87 mm Hg, 95% CI:−4.14 to 0.41) was found from 12 to 24 months. No significant changes were observed for other clinical outcomes. Further analysis showed that the percentage of patients who achieved A1c <7.0% increased from 3.1% before health literacy intervention to 20.6% at 12 months, and to 22.5% at 24 months (data not shown in the table).
Effect of health literacy and exercise interventions on clinical outcomes in patients with diabetes
In the exercise group, DID analysis indicated that 1-year exercise intervention yielded an improvement in glycemic control, with A1c level decreasing by 0.81% (95% CI: −1.17 to −0.45), but a significant increase in LDL-C (0.21 mmol/L, 95% CI: 0.26 to 0.44). No significant change in other clinical outcomes were observed. As a result, the percentage of patients who achieved A1c <7.0% increased from 7.6% at baseline to 34.4% at 12 months, but then decreased to 29.3% at 24 months (data not shown in the tables).
DID analysis demonstrated that comprehensive intervention resulted in 0.44% (95% CI: −0.75 to −0.12) decrease in A1c level during the 1-year intervention period, but 0.38% (95% CI: 0.05 to 0.71) increase thereafter. Percentage of patients who achieved A1c <7.0% also increased from 2.7% before intervention to 16.0% after intervention and continuously increased to 20.0% during post-intervention period. No significant changes were observed for other outcomes (table 2).
As shown in figure 2, the health literacy and exercise groups had significant reductions in A1c at the 12 months (p<0.05), whereas the control group had an increase in A1c (p<0.05). The downward trend in A1c level continued in the health literacy and the exercise groups but did not reach statistical significance. While the A1c level decreased in the control group from 12 to 24 months, it increased significantly in the comprehensive group (p<0.05 for each within-group comparison).

{kind=link}
{kind=link}
Change in hemoglobin A1c (A1c) level from baseline to 12 and 24 months of follow-up in Chinese patients with diabetes.
Table 3 presents the results of sensitivity analyses. DID analyses indicated that the interventions attributed to improvements in glycemic control, with a decreased A1c in the three intervention groups. A1c level was found to decrease more in the health literacy group than in the exercise and the comprehensive groups, no matter based on the full samples or using a 1:1 neighbor with replacement radius matching PSM approach, which was consistent with the base case scenario. Sensitivity analysis also showed that LDL-C and DBP levels increased significantly from baseline to 12 months in the health literacy group.
Sensitivity analyses (difference-in-difference) for the effects of interventions on main clinical outcomes
Discussion
This study investigated the intervention-attributable effect of health literacy, exercise and comprehensive interventions on clinical outcomes in Chinese patients with T2DM using a cluster RCT design and a PSM approach in combination with DID analyses. A significant decrease in A1c level and an increase in proportion of patients achieving goal A1c were observed in all three intervention groups from baseline to 12 months, but no significant improvement in other clinical outcomes compared with the control arm. The improvement in glycemic control was higher in the health literacy group (decreased by 0.95%) than in the exercise group (decreased by 0.81%) and in the comprehensive group (decreased by 0.44%). The decreasing trend remained in the intervention groups during the 1-year post-intervention period, but did not reach significant.
Evidence in literatures was not consistent on the relationship between health literacy or numeracy levels and clinical outcomes among patients with diabetes. Several studies showed that a higher health literacy level was associated with better glycemic control,5 29–31 while more recent studies did not observe an association.32 33 This study, with a strong evidence, documented a positive association between health literacy intervention and glycemic control in Chinese patients. For exercise intervention, Umpierre et al34 found that structured aerobic exercise training was associated with an absolute A1c reduction of 0.73% compared with the control group, and structured exercise of >150 min per week was associated with an absolute A1c reduction of 0.89%. These findings were similar to our results that 12 months exercise intervention was associated with an absolute A1c reduction of 0.81%.
It was hypothesized that comprehensive intervention would be more effective than exercise or health literacy intervention alone in improving main clinical outcomes, especially glycemic control. These expected results, however, were not observed in this study. One possible explanation for the least intervention-attributable effect on glycemic control in the comprehensive group may be the decreasing adherence to the interventions among patients due to too high frequency of interventions. As suggested by the literature, adherence to intervention content and delivery explains much of the variance in effectiveness.35 With efforts to maximize program adherence, a higher intervention-attributable effect might be observed in the comprehensive group.
Health literacy and exercise interventions also improved blood pressures, but the improvement was also observed in the control arm. Our finding is in line with three previous RCTs, in which the control groups showed comparable improvements in blood pressure to those in the behavior intervention groups.36–38 Regarding the serum lipids, effect of diabetes interventions was not consistent.39 40 Twelve months of aerobic and resistance training significantly improved HDL-C, but did not change LDL-C.41 In this study, we did not observe any additional benefits in HDL-C from interventions. Even worse, we observed an increase in LDL-C in the intervention groups possible due to usage of diet module of PRIDE toolkit. It is possible that subjects receiving health literacy intervention might increase their intake of meat, eggs and beans, which are good sources of high-quality protein, and thereby had higher LDL-C level. Further analysis of the 3 days 24 hours dietary recall data showed a significant increase in dietary fat intake in the three intervention groups, but not in the control arm.
Our study has a number of important implications. From public health standpoint, our findings can inform strategic plans to address the growing T2DM epidemic and economic burden. It is suggested that reducing A1c by 0.7% can reduce microvascular complications by 40%–60%. Lowering A1c in patients with diabetes also decreases absolute risk of developing CHD by 5%–17% and all-cause mortality by 6%–15%.42 Hereby, we estimate that 1-year interventions may reduce amount of disease burdens.23 Nevertheless, these public health interventions should focus on health literacy or aerobic exercise, yet both components at the same time may diminish the effect. One-size-fits-all approach is not recommended to improve diabetes self-management. Building of the most effective intervention should base on consideration of program adherence as well as other demographic characteristic factors. For healthcare professionals, the observed positive association between health literacy, aerobic exercise and glycemic control should serve as a call for action. Education on self-management with a component of health literacy improvement and aerobic exercise, which in turn leads to better diabetes management is required at clinical level. Other strategies that improve communication and intervention adherence also need to be taken into consideration as part of the intervention. For patients themselves, improvement in knowledge of T2DM and practice of aerobic exercise can result in better glycemic control.
Limitations
Despite the strong design with cluster randomization in addition to PSM approach and DID analysis, findings of this study need to be interpreted with considerations of some limitations. First, the generalization of the results may be limited due to the small sample size (799 patients with T2DM) and highly selected patients (with most recent A1c ≥7.5% or fasting glucose ≥10 mmol/L). Second, Shanghai is one of the most economically developed cities in China, whose residents have a higher health literacy level.43 Results derived from this population may underestimate the effect of health literacy intervention in Chinese patients who are usually with low health literacy. Finally, the 2-year study period might not be long enough to allow the effect of interventions shown on occurrence of diabetes complications. Further studies are called for to document the long-term benefits of these interventions as well the effect of longer intervention.
Conclusions
With the increasing numbers of people affected by diabetes, it is essential to promote patient self-management. This study further demonstrated that all three interventions involving health literacy and exercise improve glycemic control in Chinese patients with T2DM, with a greater effect of health literacy intervention alone than the intervention with both components. Implementation of interventions with a focus on health literacy and exercise has the potential for improving diabetes management and reducing diabetes burden in China.
Acknowledgments
The authors would like to thank all patients with diabetes who participated in the study, and appreciate the efforts of staff from the Minhang CDC, Changning CDC, and eight community healthcare centers in Minhang district and Changning district in the project implementation and data collection. The authors would also like to thank the research assistants for their great contributions to data collection and data entry.
References
Footnotes
Presented at Selected content was presented as a poster at the Lancet-CAMS Health Summit, Beijing, China, October 12–14, 2017.
Contributors YW drafted the manuscript. XL, JM and LW contributed to subject recruitment, data collection and quality control. YZ, YC and YW contributed to statistical analysis and data interpretation. WX and LS involved in the conception and design of the study, data interpretation and statistical analysis. WX and RR contributed to the design of the trial. All authors critically reviewed the manuscript and have approved the publication of this final version of the manuscript. WX is the guarantor of this work and had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This study was supported by the China Medical Board (CMB) Open Competition Project (No.13-159) and the Social Science Fund of China National Ministry of Education (No. 14YJAZH092).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethics approval was obtained from the Medical Ethics Committee of Fudan University (IRB00002408 & FWA00002399, approval no. 2013-06-0451). All participants provided written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. De-identified data collected for this study and a data dictionary are available from the corresponding author on reasonable request.
Author note Reference to prior publication of study: Liu X, Fang H, Xia Q, Cheng Y, Zhou P, Yan Y, Gao J, Jiang Y, Yao B, Rothman RL, Xu WH. Effect of health literacy and exercise interventions on glycated haemoglobin levels in Chinese patients with type 2 diabetes: a cluster-randomised controlled trial. Lancet, 2017;390:S92 (Conference Abstract). Wang L, Fang H, Xia Q, Liu X, Chen Y, Zhou P, Yan Y, Yao B, Wei Y, Jiang Y, Rothman RL, Xu W. Health literacy and exercise-focused interventions on clinical measurements in Chinese diabetes patients: a cluster randomized controlled trial. EClinicalMedicine. 2019 Nov 19;17:100-211. doi: 10.1016/j.eclinm.2019.11.004. eCollection 2019 Dec.