Article Text

Abstract
The popularity of teleconsultation during the COVID-19 pandemic enabled increased accessibility for individuals with type 2 diabetes mellitus (T2DM). However, previous studies did not distinguish between synchronous and asynchronous teleconsultation. We evaluated the effectiveness of synchronous teleconsultation for patients with T2DM. We searched Medline, Embase, Cochrane Central Register of Controlled Trials, Cochrane Library and Cochrane Database of Systematic Reviews, ClinicalTrials.gov, and the WHO International Clinical Trials Registry Platform databases from inception to July 2021. All included studies were randomized controlled trials of synchronous teleconsultation for adults with T2DM compared with usual care. Reviewers independently extracted data and used the Cochrane tool to evaluate risk of bias. Meta-analyses were conducted using random-effects models. A pooled mean difference for both HbA1c (%) and body mass index (BMI) (kg/m2), systolic blood pressure (SBP) (mm Hg), diastolic blood pressure (DBP) (mm Hg), and low density lipoprotein cholesterol (LDL-cholesterol) (mg/dL) were calculated. Patient-reported outcomes, such as depression, medication adherence, and quality of life, were also assessed. A total of 9807 abstracts were identified and 27 trials were included. Synchronous teleconsultation significantly resulted in greater decrease in HbA1c compared with usual care group (n=8746, 0.35, 95% CI 0.20 to 0.49, I2=73%, p<0.001). No significant effects on BMI (n=699, 0.08 kg/m2, 95% CI −0.54 to 0.69), SBP (n=5512, 1.32 mm Hg, 95% CI -0.09 to 2.73), DBP (n=2898, 0.17 mm Hg, 95% CI −1.18 to 1.52), or LDL-cholesterol (n=5276, 3.21 mg/dL, 95% CI −1.75 to 8.17) were found. The effect of teleconsultation in improving patient-reported outcomes was uncertain. Thus, synchronous teleconsultation could be an alternative to usual care. Systematic review registration is PROSPERO CRD42021267019.
- Meta-Analysis
- Dietetics
- Telemedicine
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Diabetes mellitus is a critical global health issue, and the prevalence is projected to increase in the coming decades. Approximately 422 million people worldwide have diabetes, with the majority residing in low-income and middle-income nations. Diabetes is directly responsible for 1.5 million fatalities annually.1 People who have type 2 diabetes mellitus (T2DM) frequently deal with complications that might lower their quality of life and increase their mortality.2
Due to the Coronavirus disease (COVID-19) pandemic, persons with T2DM were encouraged to adopt telemedicine as an alternative for challenges in diabetes management because of social distancing requirements. Telemedicine is the use of medical data sent between places via electronic communications to improve a patient’s clinical health state, according to the American Telemedicine Association. There are an increasing number of telemedicine-related applications and services that use two-way videos, smartphones, wireless devices, and other types of telecommunications technology.3
According to a previous review, the most effective telemedicine technique is teleconsultation.4 Teleconsultation is a two-way conversation between caregivers and one or more patients using a variety of communication and information technologies (automated messaging system, email, internet, phone, or other devices without actual face-to-face interaction).4 In order to prevent or delay complications and optimize patients’ quality of life, the intervention involves offering healthcare, such as providing education on problem-solving skills for all aspects of diabetes, exercise or medication adjustment, and so on.5 There are two types of teleconsultation: (1) asynchronous teleconsultation, which involves monitoring and delivering feedback exclusively via short message service text messaging, email, internet/web-based platforms, home gateway, server, or post; and (2) synchronous teleconsultation, which involves real-time video interactions between physician(s) and patient(s) (via videoconferencing equipment of videophone, television, digital camera, webcam, and so on) and real-time audio interactions (synchronous telephone coaching and counseling that link a number of patients and healthcare professionals at once).6 7
Data from several studies have suggested that teleconsultation was not able to reduce HbA1c in patients with T2DM, when compared with usual care. Verhoeven et al, reported that pooled reduction in HbA1c through teleconsultation was not statistically significant.8 Similarly, another review by Verhoeven et al reported that pooled data from 15 randomized controlled trials (RCTs) on teleconsultation did not demonstrate a significant decrease in HbA1c when compared with conventional care (−0.10, 95% CI −0.39–0.18; I2=81%, p<0.001).6 However, a meta-analysis conducted by Zhai et al revealed a significant, although slight, decrease in HbA1c in their teleconsultation group, compared with their conventional care group (−0.37, 95% CI −0.49–0.25; I2=75.5%, p<0.001).9 According to another network meta-analysis, teleconsultation was significantly more effective over conventional care at lowering HbA1c (−0.64, 95% CI −3.74 to −0.02; I2=98%).4
The teleconsultation in the above studies did not distinguish between synchronous and asynchronous, making it difficult to assess specific effects of the different intervention types. During synchronous teleconsultations, doctors and patients can converse in real-time, ensuring the security and interaction of doctor-patient communication, which is most similar to usual care. Therefore, we conducted a systematic review and meta-analysis to assess the effectiveness of synchronous teleconsultation of included studies.
Methods
This systematic review followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and was registered in the PROSPERO database (CRD42021267019).10
Eligibility criteria
We considered studies eligible for inclusion if they were RCTs, involved adult participants (≥18 years) who were diagnosed with T2DM and used synchronous teleconsultations delivered by health professionals, regardless of treatment, patient education, and lifestyle modification coaching. The study’s setting and period or length of follow-up were unrestricted. We did not include studies in which the participants were under the age of 18 or were diagnosed with type 1 diabetes mellitus (T1DM) or gestational diabetes mellitus (GDM). Asynchronous teleconsultation was excluded, as was a control group if it used telemedicine in any way or if its primary outcomes did not include HbA1c.
Search strategy
We searched the following databases from inception to July 2021 to identify eligible RCTs: MEDLINE (Ovid SP), Embase (Ovid SP), Cochrane Central Register of Controlled Trials (CENTRAL), Cochrane Library (Wiley), and Cochrane Database of Systematic Reviews . We also searched ClinicalTrials.gov (https:// clinicaltrials.gov/) and the WHO International Clinical Trials Registry Platform (https:// www.who.int/clinical-trials-registry-platform). There were no language restrictions. We emailed the corresponding author of any ongoing or unpublished RCTs to get pertinent information. In order to check for duplicate entries automatically, we uploaded search results into the reference management software Endnote X9 (Clarivate Plc, London, UK).11 Once duplicate research had been eliminated, Endnote X9 was used to screen the titles and abstracts. Additional articles were identified by searching the references of previous studies and systematic reviews.
Study selection
Four reviewers (KL, MY, JXZ, and JYX) first reached consensus on how to apply the eligibility criteria before individually reviewing the titles and abstracts of the retrieved records in accordance with the pre-established eligibility criteria. Any disagreements were settled through discussion or by consensus if necessary. At every step of the study selection process, the number of titles or abstracts chosen and the causes of exclusion were recorded. Four reviewers (KL, MY, JXZ, and JYX) independently retrieved the full texts of all potentially pertinent articles and evaluated them for selection. The total number of full-text articles selected and reasons for exclusion were documented.
Data collection
The study characteristics extracted were document-unique identification code, article title, year of publication, National Clinical Trial number, study funding source, setting, number of participants in each group, sex distribution participants in each group, mean age±SD of each group, details of the interventions in each group (ie, by what type of healthcare provider, what kind of medium, and frequency of the intervention), length of intervention, primary outcomes (HbA1c, body mass index (BMI), systolic blood pressure, diastolic blood pressure, LDL-cholesterol), and secondary outcomes (depression, quality of life, diabetes distress, self-efficacy, medication adherence). We emailed the study’s first or corresponding author to ask for more information when there were data gaps or areas of uncertainty.
Risk of bias (quality) assessment
Using the Cochrane risk of bias tool for RCTs, we evaluated the risk of bias and classified each trial as having a low, high, or unclear risk of bias for each area. Six bias domains are included in the tool: selection (random sequence generation and allocation concealment), performance, detection, attritions, reporting, and other biases.12 Each trial’s risk of bias was evaluated independently by four reviewers (KL, MY, JXZ, and JYX). In the event of a disagreement, consensus decision-making was used to achieve the most agreeable decision to all.
Strategy for data synthesis
We conducted our meta-analyses using Review Manager 5.4.1 (Cochrane Collaboration, London, UK).13 Our choice of random effects models was based on our expectation of a variety of intervention components and comparator conditions leading to a wide range of treatment effects. For each analysis, the pooled mean difference was calculated, and I2 and τ2 statistical tests were used to compare the variation in study heterogeneity. Where secondary outcome assessments were methodologically heterogeneous, we narratively summarized the findings. Based on a careful review of the both the included studies and previous reviews, we estimated that heterogeneity was mostly due to differences in interventions. A subgroup analysis was possible for the type of healthcare provider, teleconsultation medium, and frequency of teleconsultations.
Type of healthcare provider
We compared different healthcare provider subgroups based on the extracted data, including nurses,14–24 therapists,25–28 and non-medical practitioners (eg, health educators).29–31 Teleconsultations were found to be provided by a variety of healthcare practitioners. In the subgroup analysis of practitioner delivery, we designated this group as “other” if it was unclear whether a nurse or dietician provided the intervention.
Teleconsultation medium
We explored the effectiveness of interventions according to the medium (telephone or videoconference) used.
Frequency of teleconsultation
We extracted data on the number of times and duration of teleconsultation and calculated the monthly intervention frequency. As the median monthly intervention frequency was one, we categorized the intervention group according to whether the monthly intervention frequency was ≥1 or <1.
Results
Study selection
After eliminating duplicates, 9807 unique study titles or abstracts were identified for this systematic review (figure 1). From 101 potentially eligible full-text articles, 81 studies were excluded because 9 involved patients with other conditions (eg, T1DM or GDM), 4 were not RCTs studies, the intervention in 16 trials was not synchronous teleconsultation, 6 were duplicated records, 38 were review articles and 9 did not report HbA1c as outcomes. Eight new trials met the inclusion criteria from the systematic reviews. Finally, we identified 27 studies eligible for inclusion in this systematic review.14–40 After data extraction and further screening, we identified 23 studies containing sufficient non-overlapping HbA1c data suitable for meta-analysis.14–31 34 35 37–39 figure 1 depicts a PRISMA flow diagram detailing the study selection process.
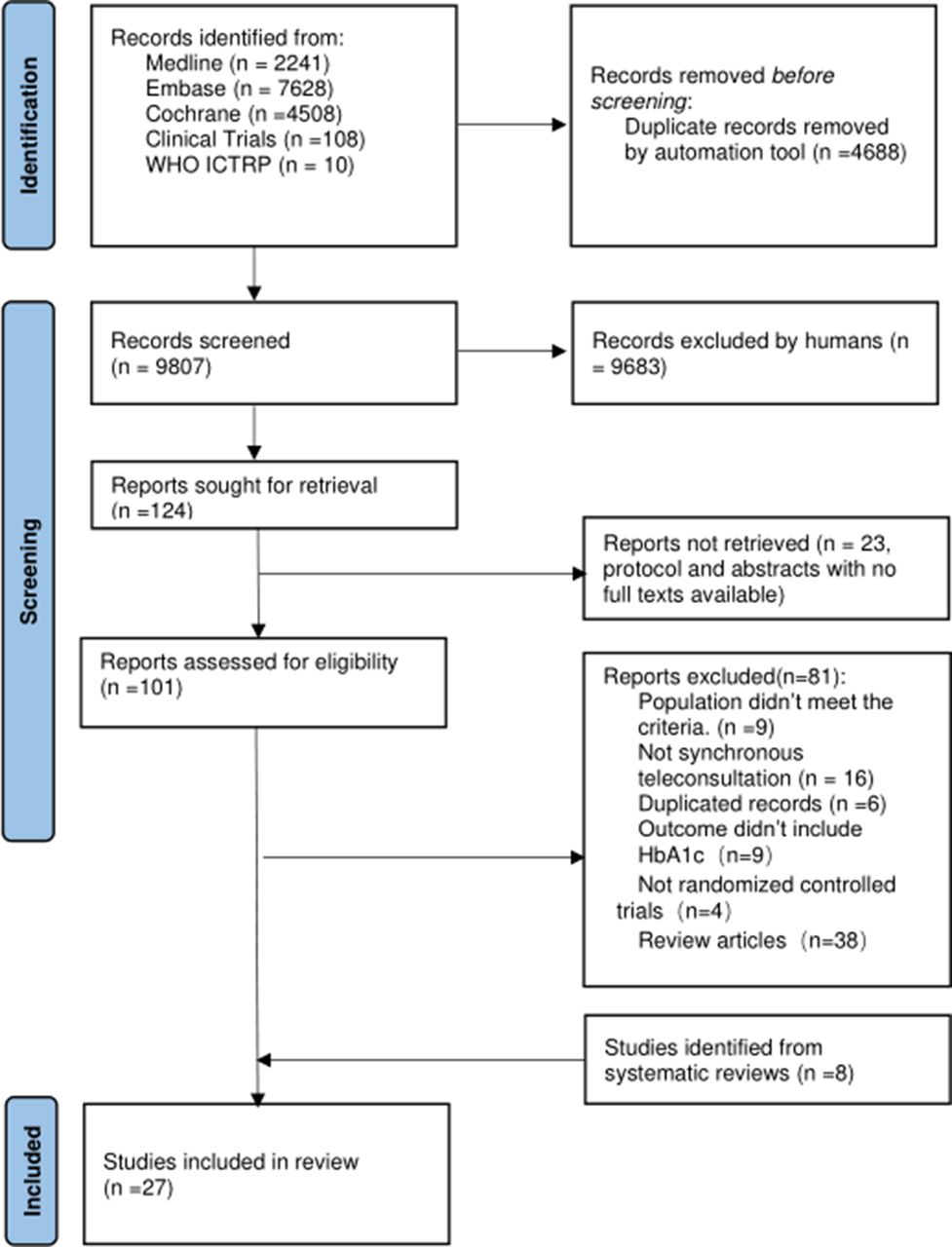
PRISMA diagram for the literature search. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Quality assessment
We considered a study to have a low risk of bias if at least four of the seven total components in it were classified as having a low risk of bias. 18 trials had a low risk of bias, while 9 studies had a high risk. The risk of bias graph and risk of bias summary are provided in online supplemental figures 4 and 5.
Supplemental material
Study characteristics
Characteristics of included trials
All included trials were individual RCTs. A total of 10 019 patients were included in these trials. Studies were carried out in the USA (n=10), South Korea (n=4), Australia (n=3), Denmark (n=3), Germany (n=1), Iran (n=1), Spain (n=1), Turkey (n=1), the UK (n=1), Ghana (n=1) and China (n=1) in terms of geographical representation. Interventions occurred in secondary or territory care settings (n=14)and in primary care (n=13) (see table 1).
Characteristics of included trials (n=27) ordered chronologically
Type and duration of intervention
The providers of teleconsultation intervention in the trials were nurses (n=11), therapists (n=4), and non-medical practitioners (n=3). The teleconsultation intervention in 10 trials focused on education and reinforcement of diet, 9 trials aimed at exercise adjustment, 13 trials concentrated on medication adherence and 11 trials focused on self-monitoring of blood glucose levels. Eighteen (18) trials provided teleconsultation via the telephone, and 9 trials through video conferences. The total length of intervention in 14 trials was>6 months, and in 11 trials was≤6 months. The frequency of intervention in 14 trials was more than once monthly on average, and in 6 trials was less than once monthly on average (see online supplemental table 1).
Measurement of outcomes
The following clinical outcomes were evaluated in the majority of studies: HbA1c (27 trials), BMI (5 trials), systolic blood pressure (13 trials), diastolic blood pressure (11 trials), and LDL-cholesterol (7 trials). Several different validated questionnaires were employed to assess patients’ depression (2 trials), quality of life (2 trials), diabetes distress (1 trial), self-efficacy 1 trial), and medication adherence (4 trials) (see table 1) .
The questionnaires were as follows:
The PHQ-9 (two trials).
The Problem Areas in Diabetes Scale (one trial).
The Short Form 36, version 1 (one trial).
Diabetes Management Self-Efficacy Scale (one trial).
The Assessment of Quality of Life (one trial).
Effectiveness of synchronous teleconsultation delivered by healthcare practitioners on clinical outcomes in patients with T2DM
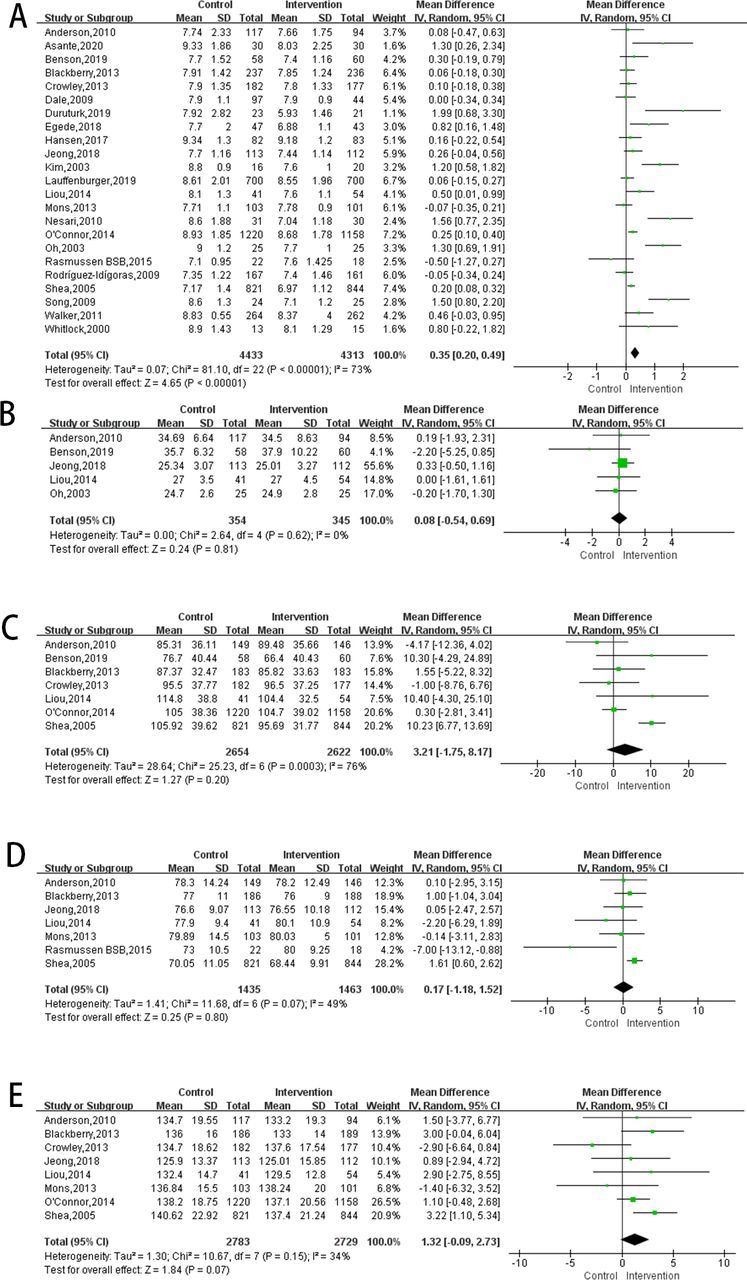
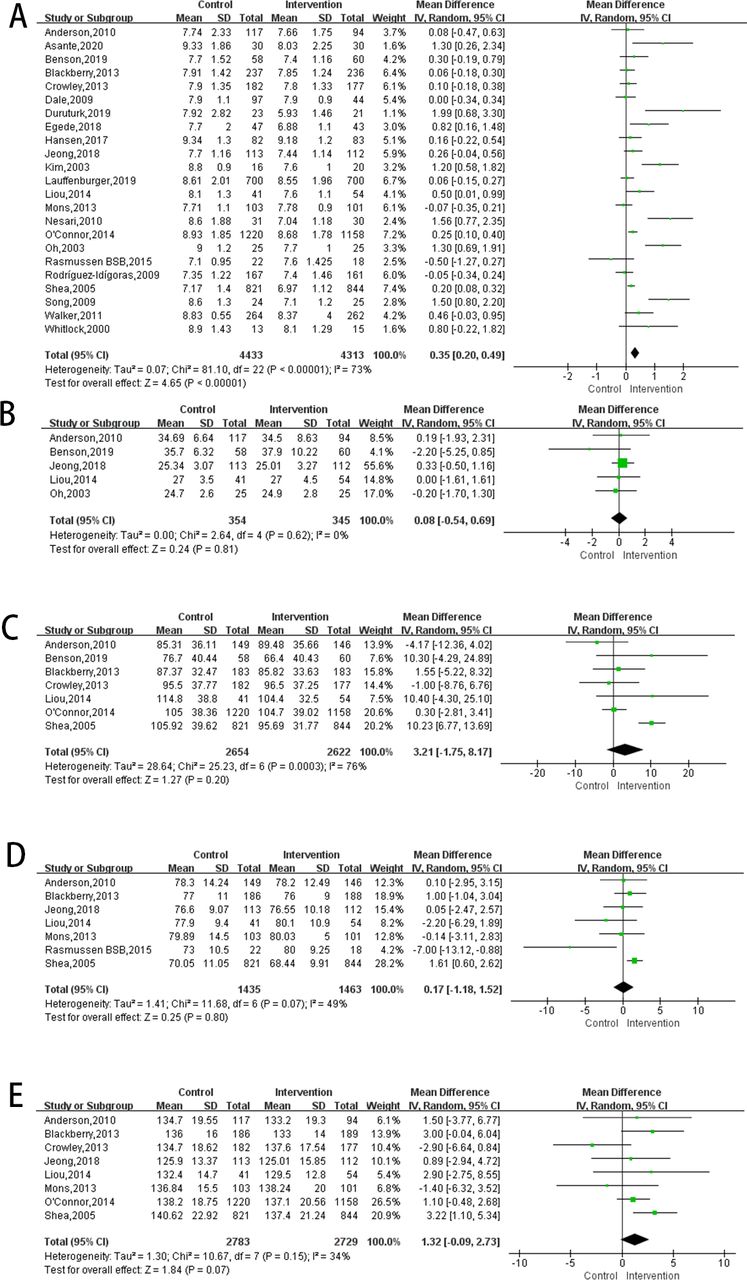
A small difference was found at the meta-analysis level in HbA1c when comparing the synchronous teleconsultation group with the conventional care group. The mean difference in HbA1c was 0.35 (95% CI 0.20 to 0.49; I² = 73%; τ2=0.03, p<0.001) in favor of the intervention. HbA1c levels were measured in 27 RCTs, but only 23 were suitable for meta-analysis. Subgroup analyses were also conducted. We found no statistical significance for BMI, LDL-cholesterol, or systolic and diastolic blood pressure at the meta-analysis level (figure 2).
{kind=link}
{kind=link}
Forest plot of comparison: HbA1c, BMI, LDL-cholesterol, DBP, SBP. (A) Forest plot of comparison: HbA1c. (B) Forest plot of comparison: BMI. (C) Forest plot of comparison: LDL-cholesterol. (D) Forest plot of comparison: DBP. (E) Forest plot of comparison: SBP. BMI, body mass index.
Subgroup analyses results for HbA1c
Type of healthcare provider
Differences found in subgroup analyses of the type of provider in HbA1c were not statistically significant (p=0.29). The mean difference between interventions provided by non-medical practitioners (such as health educators) was 0.66 (95% CI 0.10 to 1.22; I2=71%; τ2=0.17). Therapist-led interventions had a mean difference of 0.46 (95% CI 0.02 to 0.90; I2=76%; τ2=0.13) and the mean difference for nurse-delivered interventions was 0.37 (95% CI 0.12 to 0.61; I2=79%; τ2=0.11). The mean difference for the group of “other” practitioners was 0.18 (95% CI −0.03–0.38; I2=45%; τ2=0.02) (online supplemental figure 1).
Synchronous teleconsultation medium
There was no significant difference (p=0.79) between subgroups of synchronous teleconsultation media in HbA1c. Participants who received synchronous teleconsultation over telephone (mean difference of 0.37, 95% CI 0.18 to 0.57; I2=78%; τ2=0.10) were found to have similar results to those who received it through videoconference (mean difference of 0.33, 95% CI 0.09 to 0.57; I2=78%; τ2=0.10) (online supplemental figure 2).
Frequency of synchronous teleconsultation
There were significant differences found in this subgroup (p<0.01) when exploring the effects of synchronous teleconsultation frequency in HbA1c. Significantly larger reductions in HbA1c were achieved with a higher monthly intervention frequency (≥1) (mean difference 0.67, 95% CI 0.40 to 0.94; I2=79%; τ2=0.17, p<0.01) whereas there was no discernable difference found between the comparator and intervention groups in the lower monthly intervention (<1) group (mean difference 0.10, 95% CI −0.04–0.24; I2=18%; τ2=0.01, p=0.30) (online supplemental figure 3).
Through subgroup analysis, only the lower monthly intervention frequency (I2<25%) was found to partially explain the cause of heterogeneity.
Effectiveness of synchronous teleconsultation on patient-reported outcomes
Depression
Two studies reported on depression.14 16 There were no group differences found in these two studies.
Medication adherence
Four studies reported on medication adherence. Three studies found significant differences between groups,15 21 27 whereas one study did not find any between-group difference.28
Quality of life
Two studies reported on quality of life.16 18 Both studies found no difference between groups.
Discussion
Worldwide, governments are trying to identify an alternative method to assist persons in managing T2DM as effectively as usual care. We evaluated the effectiveness of synchronous teleconsultation for patients with T2DM in this systematic review. For the primary outcomes, we found that synchronous teleconsultation delivered by health professionals resulted in greater HbA1c reduction compared with usual care. Patient management is important to improve HbA1c levels.41 However, continuity of patient management in usual care is often not ensured due to time or space constraints.15 Synchronous teleconsultation offers the possibility of patient management outside the clinic, enabling patients to better self-manage regarding exercise, blood glucose monitoring, diet planning, and medication adjustment according to the guidance of medical staff. This may be the cause of why synchronous teleconsultation is more successful than usual care at lowering patients’ HbA1c.
Evidence suggests that non-medical practitioners or nurses may be able to deliver synchronous teleconsultations just as successfully as therapists, as both showed statistically significant HbA1c decreases. It is possible that nurses or non-medical practitioners are also sufficiently certified in standard diabetes management and teleconsultation techniques.16 19 29 Our findings suggest that nurses and non-medical practitioners could be selected to provide teleconsultations to ease the burdens of physician, who often deal with major time constraints. Many studies have shown that treatment adjustments managed by nurses and non-medical practitioners mirrored recommendations by patients’ general physicians.16–21 23 30 34 38 A lack of focus on drug-based interventions by practice nurses may be attributed to discomfort or lack of confidence in their ability to interfere with the patient and doctor’s current therapeutic management.16 Therefore, when synchronous teleconsultations are run by nurses, they should be supervised by doctors when adjusting drug prescriptions. All synchronous teleconsultation methods showed statistically significant reductions in HbA1c, therefore both telephone and videoconference applications are encouraged. However, some teleconsultation devices, especially for videoconferences, are difficult to use, necessitating patient training. Videoconferencing equipment included in this review included a videophone, television, digital camera, and webcam, and so on. Equipment that is too challenging to operate will increase the treatment burden on patients and negatively affect the intervention effect. Increased teleconsultation frequency between patients and medical professionals resulted in a lower HbA1c level, and interventions should be planned to occur at least once a month (by telephone or videoconference).
The meta-analyses in our study revealed statistically significant heterogeneity, and our prespecified subgroup analyses accounted for some, but not all variances, suggesting that any data at the population level should be cautiously interpreted for specific patients when generating individualized decision-making. Synchronous teleconsultation for diabetes care usually involves an integrated interaction between the patient and the healthcare provider. This interaction includes diagnosis education, diet and exercise instructions, blood glucose monitoring, and medication adjustments, all of which are of importance to patients. Thus, teleconsultation is a complex intervention, and the heterogeneity of the studies included in this meta-analysis is significant, as previous meta-analyses have also demonstrated.4 6 8 In terms of complex intervention, usually as a whole-package practice, this highlights the interactive relationship between healthcare providers and patients, which is non-standard and takes on different forms in different contexts.42 It is believed that the complexity of teleconsultation resides in the components of the interaction. These include the behaviors required for delivering or receiving the consultation, the persons involved in the intervention, the outcomes concerned, and the flexibility of tailoring of the intervention. The heterogeneity of the trials included in this systematic review and meta-analysis thus seems obvious and inevitable. The issue of how to evaluate its complexity remains a challenge for researchers. Future studies should focus on creating patient-centered technologies that are tailored to each user’s requirements and abilities. Targeted users must be involved in the creation of individualized interventions through a participatory design approach.
Meanwhile, it was unclear whether synchronous teleconsultation for T2DM care was successful in enhancing other primary outcomes, for example, BMI, blood pressure, and lipids. We discovered no statistical significance for BMI, LDL cholesterol, systolic, and diastolic blood pressure at the meta-analysis level. This result did not agree with those of previous related studies,43 44 probably because the patients’ enrollment criterion was T2DM and most of the interventions focused on reducing HbA1c with much less attention on BMI, LDL-cholesterol, systolic and diastolic blood pressure, thereby resulting in poor intervention effects. Studies included in this systematic review employed more than five questionnaires for the secondary outcomes, although sometimes the same uniform questionnaire was used. Direct between-study comparisons for these outcomes were therefore not possible.
Most of the interventions excluded individuals diagnosed with T1DM, GDM, and comorbidity. These populations could also gain from synchronous teleconsultation, although we are unsure if the intervention would work in this demographic. In the past, teleconsultations with patients have been associated with weaker sympathetic communication and less direct physical touch with the patient.45 We need to assess the implementation process (eg, which patients stick with it and which give up) and communication quality more extensively. Regarding how teleconsultations may affect healthcare spending and utilization, there is still a great deal of ambiguity, especially in cases where the financial structure may be encouraging the use of low-value healthcare services.
Strengths and limitations of this review
Our conclusions are based on a large cohort (10 019 participants), and 7/27 of these trials were published after 2016. All included trials investigated laboratory results self-reported outcomes. In diabetes management programs, dropout rates must be considered since patients who receive fewer consultations are less likely to be followed up with. The limitations of our findings are worth noting in several areas. First, the included trials were primarily undertaken in socially and economically developed areas; thus, our conclusions may not be generalizable to all areas. Second, external validity was limited by significant heterogeneity between studies. The reason for this may be the variation in the type of medium, healthcare providers, frequency, and duration of teleconsultations. Previous reviews have also mentioned participant variations in sex, age, and T2DM duration. Therefore, although we can confidently conclude that synchronous teleconsultation helped lower HbA1c in patients with T2DM better than conventional care, identifying patient subgroups for whom the intervention is most useful is still challenging and requires additional research. Last, no study included in this analysis was able to successfully blind its participant side of the trial. Blinding both patients and healthcare professionals is impossible given the nature of the intervention. The introduction of this potential bias may have had an impact on the overall quality of the systematic review as well as on the individual studies.
Conclusion
The increased application of synchronous teleconsultation during COVID-19 provided greater medical access for persons with T2DM. This systematic review found that synchronous teleconsultation for healthcare givers helped lower HbA1c better than usual care group in patients with T2DM. Our findings are based on a mixture of medical professionals and different contents of teleconsultation. Interventions should consist of ≥1 contact monthly. Remote consultation can be either audio-based or video-based. Most studies were carried out in high-income countries, interventions were varied, and a variety of therapeutic areas were covered. The stated effectiveness of synchronous teleconsultations may not be generalizable across clinical contexts or treatments due to country-specific variances in health systems.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We would like to thank Editage (www.editage.cn) for English language editing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MY, CC, and KL made significant contributions to the conceptualization and methodology. Significant contributions were made to the data analysis, paper writing, and manuscript interpretation by MY, JZ, XJ, and KL. Study identification, study selection, data extraction, and assessment were the main tasks MY, KL, JZ, JY, and XJ were responsible for. JZ and XJ are cofirst authors of the article. CC are the guarantors of the entire material, will assume all liability for the research and/or conduct, will have access to the data, and will have authority over the publishing decision.
Funding Peking University Baidu Fund 2019BD018.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.