Article Text

Abstract
Objective Incident diabetes mellitus (DM) is important to recognize in patients with acute myocardial infarction (AMI). To develop an efficient screening strategy, we explored the use of random plasma glucose (RPG) at admission and fasting plasma glucose (FPG) to select patients with AMI for glycosylated hemoglobin (HbA1c) testing.
Design, setting, andparticipants Prospective registry of 1574 patients with AMI not taking glucose-lowering medication from 24 US hospitals. All patients had HbA1c measured at a core laboratory and admission RPG and ≥2 FPGs recorded during hospitalization. We examined potential combinations of RPG and FPG and compared these with HbA1c≥6.5%—considered the gold standard for DM diagnosis in these analyses.
Results An RPG>140 mg/dL or FPG≥126 mg/dL had high sensitivity for DM diagnosis. Combining these into a screening protocol (if admission RPG>140, check HbA1c; or if FPG≥126 on a subsequent day, check HbA1c) led to HbA1c testing in 50% of patients and identified 86% with incident DM (number needed to screen (NNS)=3.3 to identify 1 case of DM; vs NNS=5.6 with universal HbA1c screening). Alternatively, using an RPG>180 led to HbA1c testing in 40% of patients with AMI and identified 82% of DM (NNS=2.7).
Conclusions We have established two potential selective screening methods for DM in the setting of AMI that could identify the vast majority of incident DM by targeted screening of 40–50% of patients with AMI with HbA1c testing. Using these methods may efficiently identify patients with AMI with DM so that appropriate education and treatment can be promptly initiated.
- Diagnosis
- Myocardial Infarction
- Glucose
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
-
In a large, multicenter US cohort, we identified two potential selective screening methods for the detection of diabetes in the setting of an acute myocardial infarction using blood glucose levels collected as part of routine clinical care.
-
These screening protocols required testing glycosylated hemoglobin in only 40–50% of patients with myocardial infarction and yet identified the vast majority of those with incident diabetes—an attractive strategy for clinical and economic reasons.
-
Since patients with both myocardial infarction and diabetes are at high risk for recurrent cardiovascular events and the microvascular complications of diabetes, identification of patients with diabetes during the acute hospitalization is important, so these individuals can be targeted for more intensive lifestyle and medical interventions.
Type 2 diabetes mellitus (DM) is present in approximately one-third of patients hospitalized with an acute myocardial infarction (AMI)1 ,2 and is associated with an increased risk of short-term and long-term mortality.3 ,4 Furthermore, approximately one-quarter of patients with coronary artery disease have undiagnosed DM.5 ,6 Recognizing these patients is important, as identification of metabolic abnormalities at the time of AMI may allow for initiation of lifestyle modification, DM education, pharmacological therapy prior to discharge or referral to endocrinologists for outpatient follow-up. In addition, the presence of DM informs clinical decision making for cardiovascular care, such as revascularization options and selection and titration of selected cardiovascular medications. Introducing care strategies at the time of discharge may have the greatest likelihood of being implemented by the patient.7 ,8
Diagnosing DM during an AMI has potential challenges, however, as adrenergic and other counter-regulatory changes that occur with an AMI are associated with substantial dysregulation in glucose levels.9 For this reason, oral glucose tolerance testing, which is more reliable than glucose levels in the setting of AMI, had been previously recommended for screening of DM among patients with AMI.10 ,11 However, this method of screening can be inconvenient and is rarely used clinically in the USA, particularly during acute hospitalizations. Recently, glycosylated hemoglobin (HbA1c) testing, which is generally unaffected by transient perturbations in blood glucose and does not require fasting samples, has emerged as a new and more convenient standard for the diagnosis of DM.
While screening all patients with AMI with HbA1c is a potentially attractive strategy to detect incident DM, more selective strategies can identify the vast majority of patients with DM and be more cost-efficient.12 In addition to their clinical implications, identifying blood glucose cut-points that can accurately identify patients with DM would also be useful for research purposes; for example, in data sets where a surrogate definition of DM is needed due to missing or unmeasured HbA1c values. As such, we used a multicenter AMI registry with core laboratory-assessed HbA1c to explore different potential definitions of DM based on various fasting and random glucose cut-points, to determine if there were particular combinations of these that would be a useful initial screen for DM during AMI.
Methods
Study population and protocol
Details of the Translational Research Investigating Underlying disparities in acute Myocardial infarction Patients’ Health status (TRIUMPH) registry have been previously described.13 In brief, eligible patients had biomarker evidence of myocardial necrosis and additional clinical evidence supporting the diagnosis of an AMI. Baseline data were obtained through chart abstraction and a structured interview. All enrolled patients were asked to participate in a laboratory substudy, and consenting patients had a fasting blood specimen collected just prior to discharge, which was analyzed by a core laboratory (Clinical Reference Laboratory, Lenexa, Kansas, USA). Blood was analyzed for HbA1c, glucose and insulin levels, and lipids, the results of which were blinded to clinicians. Core laboratory HbA1c was assessed with the Bio-Rad VARIANT II assay, which is certified by the National Glycohemoglobin Standardization Program and standardized to the Diabetes Control and Complications Trial reference assay. Chart-derived HbA1c levels were not used in this study to ensure consistency and reliability of the HbA1c diagnosis of DM.
Laboratory values drawn for clinical purposes were also recorded, which included a random glucose (random plasma glucose, RPG) on admission and up to three chart values of fasting glucose (fasting plasma glucose, FPG), which were measured on venous plasma samples (ie, capillary blood glucose measurements were not collected). If a patient had >3 FPGs analyzed during the hospitalization, the first three were recorded. No other RPG values (beyond the admission value) were recorded for the hospitalization. To ensure we had a consistent patient population, all included patients were required to have an HbA1c analyzed at the core laboratory and chart-derived values for an RPG on admission and ≥2 FPGs. As glucose-lowering medications could interfere with the association between HbA1c level and glucose levels, patients who were on glucose-lowering medications at admission were excluded. Use of inpatient glucose-lowering medications was not considered. Each participating hospital obtained Institutional Research Board approval, and all patients provided written informed consent.
Analytic plan
We evaluated various definitions for DM, based on FPG and RPG (at admission), using HbA1c ≥6.5% as the gold standard for diagnosis per the American Diabetes Association guidelines.14 Potential definitions included the following: (A) RPG >140 mg/dL; (B) RPG >180 mg/dL; (C) RPG ≥200 mg/dL; (D) ≥1 FPG levels ≥126 mg/dL; (E) ≥2 FPG levels ≥126 mg/dL; (F) ≥1 FPG levels >140 mg/dL; (G) ≥2 FPG levels >140 mg/dL; (H) ≥1 FPG ≥126 mg/dL and RPG ≥200 mg/dL; and (I) ≥1 FPG >140 mg/dL and RPG ≥200 mg/dL. The various thresholds for FPG and RPG were selected based on prior guidelines14 ,15 and on prior studies examining the association of stress hyperglycemia with mortality.9 For each of these definitions, we calculated the sensitivity, specificity, positive-predictive (PPV) and negative-predictive values (NPV), and accuracy (% of true results (i.e., (true positives+true negatives)/total)) for the diagnosis of DM, as defined by an HbA1c ≥6.5%. We also examined the impact on screening volume and DM recognition using two-step screening processes, which included an initial screen based on RPG at admission (with 2 thresholds, per definitions A or B) followed by screens based on FPGs on subsequent days of hospitalization (per definition E). Finally, in a sensitivity analysis, as confirmatory HbA1c testing is recommended prior to a diagnosis of DM, we examined the screening strategies among patients with an HbA1c ≥6.5% (by our core laboratory) and an additional HbA1c laboratory value (drawn at the local hospital for clinical purposes) of ≥6.5%. All analyses were conducted using SAS V.9.4 (SAS Institute, Inc, Cary, North Carolina, USA).
Results
Study population
Among 4340 patients with AMI enrolled in TRIUMPH, 952 were excluded due to the use of glucose-lowering medications, 1156 did not consent to the laboratory substudy and thus did not have core HbA1c levels, and 658 were missing the minimum number of fasting and/or random glucose measurements. The final analytic cohort thus included 1574 patients with complete data available. Patients who were excluded due to non-participation in the laboratory substudy or missing chart data were generally similar to those included in the study, although excluded patients were slightly older, more likely to be non-white, and to present with a non-ST-elevation AMI (eTable 1). However, among patients with some (but not complete) laboratory values available (n=1136 for HbA1c; n=1012 for FPG), HbA1c levels and FPG levels were qualitatively similar between those excluded and included in the analytic sample.
The demographic, clinical, and metabolic factors of the analytic population are shown in table 1. Overall, the mean age of the patients included in the final analytic cohort was 58 years, 70% were male, 72% were white, and 50% presented with ST-elevation AMI. Among the 1574 patients with AMI not on glucose-lowering medications, mean HbA1c was 6.1%±1.4%, and 18% had HbA1c ≥6.5%. The mean of the highest FPG during the hospitalization was 128 mg/dL. The percentages of patients meeting each proposed definition of DM based on RPG and FPG are shown in table 2.
Baseline demographic and clinical characteristics
Reliability of different potential definitions of diabetes, using HbA1c ≥6.5% as the gold standard
Sensitivity, specificity, PPV, and NPV of different diagnostic approaches
The sensitivity, specificity, NPV, PPV, and accuracy of the 9 potential diagnoses for DM are shown in table 2. Definitions A (RPG >140 mg/dL), D (≥1 FPG ≥126 mg/dL), and F (≥1 FPG ≥140 mg/dL) all had reasonably high sensitivity for an HbA1c ≥6.5%, and not exceeding these thresholds had high NPVs for excluding DM, and could be used for initial screening, as they would result in very few false-negatives. Using definition D (the highest sensitivity among definitions) alone as a trigger for HbA1c testing would require HbA1c testing of 36% of the AMI population and identify 78% of patients with DM, with a number needed to screen of 2.6 patients with AMI to identify 1 case of DM.
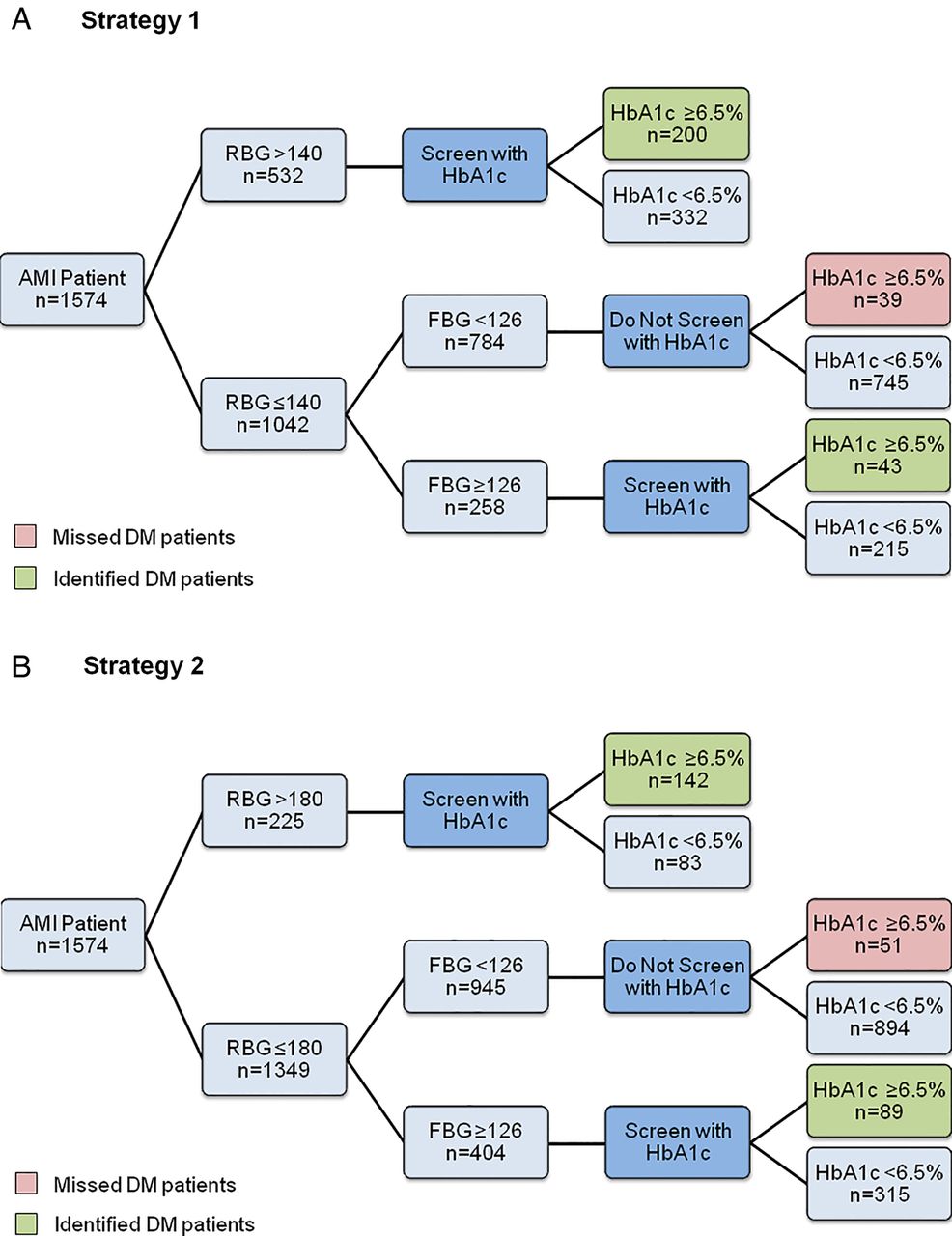
In order to maximize the number of patients with DM identified with a strategy that would fit with clinical care, we combined an initial screen with RPG on admission with screens by FPG on subsequent hospitalization days (figure 1). The first strategy (strategy 1; figure 1A) uses an RPG on presentation of >140 mg/dL as the initial trigger for HbA1c check. If on-arrival RPG was <140 mg/dL, then if an FPG is ≥126 mg/dL on a subsequent hospitalization day, HbA1c testing would be triggered. In our cohort, this strategy would require HbA1c testing of 50.2% of the patients with AMI and identify 86% of patients with DM in the cohort, with an NPV of 95%. The 39 patients who met diagnostic DM criteria by HbA1c who would not have been identified with this screening protocol had a median HbA1c of 6.8% (IQR 6.5–6.9%). Alternatively, using an RPG cut-point of >180 mg/dL to trigger an HbA1c test (strategy 2; figure 1B) would require HbA1c testing of 40% of the AMI population and identify 82% of patients with DM, with an NPV of 95%. The 51 remaining, unrecognized patients with DM had a median HbA1c of 6.8% (IQR 6.5–6.9%). Comparing these two-step screening methods, strategy 1 would screen an additional 10% of AMI population to identify 4% more of the patients with DM. The number needed to screen to identify 1 case of DM would be 3.3 with strategy 1, 2.7 with strategy 2, and 5.6 with universal screening (ie, screening all patients with AMI using HbA1c). In the sensitivity analysis examining only patients who had a core and chart HbA1c level ≥6.5% (n=164), strategy 1 would identify 154 patients (94%) of those who met criteria for DM, and strategy 2 would identify 153 patients (93%).
{kind=link}
Schematic of screening program for diabetes mellitus (DM) during acute myocardial infarction (AMI). Each strategy uses a random plasma glucose (RPG) at admission greater than a defined threshold, or fasting plasma glucose (FPG) ≥126 mg/dL on any subsequent day, to trigger glycosylated hemoglobin (HbA1c) testing. (A) Strategy 1: the results using a cut-point for admission RPG >140 mg/dL by FPG for screening. (B) Strategy 2: the results using a cut-point for admission glucose of >180 mg/dL for screening. Strategy 1 has a sensitivity 86%, specificity 58%, positive-predictive value (PPV) 31%, negative-predictive value (NPV) 95%, and accuracy63%. Strategy 2 has a sensitivity 82%, specificity 69%, PPV 37%, NPV 95%, and accuracy 71%.
In the analyses designed to identify the ideal combination of blood glucose levels for diagnosing DM (ie, for research purposes in the absence of measured HbA1c levels), the most accurate estimation of the presence of DM using only RPG and FPG was similar for all definitions except A (RPG >140 mg/dL) and D (≥1 FPG ≥126 mg/dL), which were too sensitive and had very low PPVs. Definitions H and I, which include a combination of elevated RPG and FPG, had the highest PPVs and thus were least likely to falsely identify any patients as having DM. However, these definitions also missed more patients with DM.
Discussion
In a large cohort of patients with AMI, we examined several potential combinations of random and fasting glucose levels obtained during hospital admission to identify patients with DM (defined by a core laboratory HbA1c ≥6.5%). For DM screening, an RPG on arrival of >140 mg/dL or an FPG ≥126 mg/dL were both highly sensitive for identifying patients with HbA1c-defined DM. In addition, a combination of RPG on arrival (using either the cut-point of >140 mg/dL or >180 mg/dL) or an FPG ≥126 mg/dL proposed as triggers for subsequent HbA1c testing, would lead to a marked reduction in the number of screening HbA1c tests performed (40–50% of the AMI population) and would detect 82–86% of patients with incident DM. Alternatively, a single FPG ≥126 mg/dL to trigger HbA1c testing could also be used to identify the vast majority of patients with AMI with DM. Furthermore, the cohort of patients whose incident DM diagnosis would have been missed by such targeted HbA1c screening had relatively mild elevations of HbA1c; thereby potentially minimizing the impact of not recognizing these patients during their AMI hospitalizations. Finally, we identified several definitions with high accuracy that would be reasonable surrogates for the definition of DM in research studies, when HbA1c is not available.
Unrecognized DM is common in patients hospitalized with AMI.5 ,6 Accordingly, there have been efforts to diagnose DM during AMI hospitalization using oral glucose tolerance testing and HbA1c.10 ,11 European guidelines recommend screening patients with AMI with an HbA1c and/or fasting glucose and, if inconclusive, an oral glucose tolerance test.16 However, given the acute fluctuations in blood glucose during AMI,9 ,17 it is unclear what thresholds of glucose necessitate further testing. Some researchers have sought to establish risk scores for diabetes based on waist circumference, family history, age, etc,18 but these have not been routinely implemented in patients with AMI and have not been recommended by guidelines due to increased complexity beyond simply testing HbA1c. We have established two potential strategies, using routinely collected admission and FPG levels, which could be used to inform selective screening of HbA1c. Given the ubiquitous use of electronic medical records in many countries, such a protocol could also be automated, with triggers to conduct a reflex add-on HbA1c if cardiac markers are elevated, admission RPG >180 (or 140 mg/dL), or FPG ≥126 mg/dL (per morning chemistry panel), and no HbA1c measurement documented within the past 3 months. This information could not only improve the identification of new DM but would also be useful in monitoring the efficacy of glycaemic control in patients with treated DM.19 Importantly, these strategies were successful in identifying the vast majority of patients with DM while measuring HbA1c in only 40–50% of patients with AMI and reducing the number needed to screen by half. Universal HbA1c testing does have the advantage of also identifying the large proportion of patients with pre-DM (HbA1c 5.7–6.4%) who may benefit from nutritional and lifestyle counseling, and thus this strategy may be appropriate for healthcare systems without substantial testing limitations. While an HbA1c test is not prohibitively expensive, the costs associated with ‘universal’ HbA1c screening of patients with AMI are not inconsequential in resource-limited healthcare settings, where these more selective strategies (based on data already collected) may be more cost-effective.
Furthermore, we have identified several combinations of fasting and admission glucose levels that could be used as potential surrogate definitions of DM when HbA1c is not available. These are particularly useful in large studies where HbA1c levels are missing in a substantial proportion of patients. In these cases, researchers may prefer one definition over another, depending on the goals of the study. For example, if a particular project needs to assure the DM group includes only patients with DM, then a definition with very high PPV, such as H or I, would be optimal. However, if a project wants to assure the non-DM group does not include any patients with DM, then a definition with highest NPV such as A, D, or F, would be optimal. For most projects, a balance between these is desired, which is where accuracy becomes most relevant.
There are potential limitations to our study that should be considered. First, although our study represents a large and diverse group of patients with AMI from academic and non-academic US hospitals that varied with respect to size and geography, it is unclear if our results would be generalizable to non-US patients with AMI. Second, patients admitted with high glucose levels or diet-controlled DM may have been empirically treated with correctional ‘sliding scale’ insulin during their AMI, which could potentially lower their subsequent FPG levels and thus interfere with our analyses of the relationship between FPG and HbA1c levels. However, typical correctional insulin protocols would not have impacted admission RPG levels and should have minimal (if any) impact on FPG—the two metrics evaluated in our study. Third, we used HbA1c ≥6.5% as the gold standard for DM in our study, which is known to be less sensitive than oral glucose tolerance testing.10 ,11 However, it is emerging as a popular screening method for DM16 given its greater convenience in not requiring the patient to fast or complete an oral glucose tolerance test and since clinicians are accustomed to using this test for the management of DM once its presence is established. Finally, the current diagnostic criteria of the American Diabetes Association advise the confirmation of a high HbA1c with a second HbA1c test,14 which was not available in TRIUMPH. However, there were a subset of patients who had HbA1c tests drawn locally during the acute hospitalization, and 91% of these locally drawn HbA1c levels were also ≥6.5%. In addition, we performed a sensitivity analysis among those with both values and found that the screening strategies remained highly effective.
In conclusion, in a large, multicenter cohort of patients with AMI, we identified two potential selective screening methods for DM using blood glucose levels collected as part of routine clinical care. These screening protocols required testing HbA1c in only 40–50% of patients with AMI and yet identified the vast majority of those with incident DM—an attractive strategy for clinical and economic reasons. We also found several definitions that could identify patients with probable DM based on routine blood glucose levels alone, which could be useful in large-scale clinical databases for research or population screening purposes when HbA1c levels are unavailable. Since patients with AMI and DM are at particularly high risk for recurrent cardiovascular events and the microvascular complications of DM, identification of patients with DM during AMI is important, so these individuals can be targeted for more intensive educational, lifestyle, or even medical interventions for their DM. Future work evaluating the implementation of screening processes and their impact on DM identification and management is needed.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors SVA designed the study and the statistical analysis plan, analyzed and interpreted the data, and drafted and revised the paper. KJL, SEI, and MK designed the study, interpreted the data, and drafted and revised the paper. YL analyzed and interpreted the data, and drafted and revised the paper. DKM, AG, JMS, ML, and JAS interpreted the data, and drafted and revised the paper.
-
Funding TRIUMPH was sponsored by a grant from the National Institutes of Health (National Heart, Lung, Blood Institute): SCCOR Grant #P50HL077113-01. This study was sponsored by a research grant from Genentech, South San Francisco, California, USA. The funding organizations did not play a role in the conduct of the study or in the collection, management, analysis, and interpretation of the data.
-
Competing interests DKM received consultant honoraria from Takeda, Janssen, Merck, Regeneron, and Boehringer Ingelheim; and received clinical trial leadership honoraria from Boehringer Ingelheim, Takeda, Orexigen, Genentech, Roche, AstraZeneca, Bristol Myers Squibb, Eli Lilly, Daiichi Sankyo, Merck, Eisai, Omthera, Lexicon, Novo Nordisk, GlaxoSmithKline, and Janssen. JMS received grant support from GE Healthcare; consultant honoraria from Cordis Corp.; and serves on the speaker's bureau for Astra Zeneca, Astellas, and InfraReDx LLC. JAS received research grants from the NHLBI, American Heart Association, American College of Cardiology Foundation, Gilead, Lilly, EvaHeart, and Amorcyte; and received consultant honoraria from United Healthcare, Genentech, and Amgen. MK received research grants from the American Heart Association, Genetech, Sanofi-Aventis, Gilead, Medtronic Minimed, Glumetrics, Maquet, and Eisai; and received consultant honoraria from Genentech, Gilead, F Hoffmann LaRoche, Medtronic Minimed, AstraZeneca, Abbvie, Regeneron, Edwards Lifesciences, and Eli Lilly.
-
Patient consent Obtained.
-
Ethics approval Institutional Research Board at each institution in TRIUMPH.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.