Article Text

Abstract
Introduction Previous studies in mostly Western populations have yielded conflicting findings on the association of vitamin B12 with diabetes risk, in part due to differences in study design and population characteristics. This study sought to examine the vitamin B12–diabetes association in Chinese adults with hypertension by both cross-sectional and longitudinal analyses.
Research design and methods This report included a total of 16 699 participants from the China Stroke Primary Prevention Trial, with pertinent baseline and follow-up data. Diabetes mellitus was defined as either physician-diagnosed diabetes, use of glucose-lowering drugs, or fasting blood glucose (FBG) ≥7.0 mmol/L. New-onset diabetes was defined as any new case of onset diabetes during the follow-up period or FBG ≥7.0 mmol/L at the exit visit.
Results At baseline, there were 1872 (11.2%) patients with diabetes; less than 1.5% had clinical vitamin B12 deficiency (<148.0 pmol/L). Over a median follow-up period of 4.5 years, there were 1589 (10.7%) cases of new-onset diabetes. Cross-sectional analyses showed a positive association between baseline vitamin B12 levels and FBG levels (β=0.18, 95% CI 0.15 to 0.21) and diabetes (OR=1.16, 95% CI 1.10 to 1.21). However, longitudinal analyses showed no association between baseline vitamin B12 and new-onset diabetes or changes in FBG levels. Among a subset of the sample (n=4366) with both baseline and exit vitamin B12 measurements, we found a positive association between an increase in vitamin B12 and an increase in FBG.
Conclusions In this large Chinese population of patients with hypertension mostly sufficient with vitamin B12, parallel cross-sectional and longitudinal analyses provided new insight into the conflicting findings of previous studies, and these results underscore the need for future studies to consider both baseline vitamin B12 and its longitudinal trajectory in order to better elucidate the role of vitamin B12 in the development of diabetes. Such findings would have important clinical and public health implications.
- vitamin B12
- diabetes mellitus, type 2
- longitudinal studies
- hypertension
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Conflicting findings were derived from previous studies on B12 and diabetes using either cross-sectional or longitudinal design. Some cross-sectional studies found that B12 was positively associated with diabetes, while others reported the opposite results. Several longitudinal studies showed no significant relationship between B12 and DM).
To date, the relationship between B12 and DM has remained elusive.
What are the new findings?
This is the first and largest study of a Chinese population of patients with hypertension (n=16 699) to delineate cross-sectional and longitudinal associations between plasma vitamin B12 and diabetes risk.
The cross-sectional analyses showed a positive association between baseline vitamin B12 levels and diabetes; however, longitudinal analyses revealed no association. Among a subset of sample (n=4366) with both baseline and exit B12 levels, we found a positive association between an increase in B12 and an increase in fasting blood glucose.
How might these results change the focus of research or clinical practice?
Findings from our cross-sectional and longitudinal analyses underscore the need for future studies to consider both baseline vitamin B12 and its longitudinal trajectory in order to better elucidate the role of vitamin B12 in the development of diabetes.
Such findings, if further confirmed, have important clinical and public health implications.
Introduction
Diabetes mellitus (DM) is a chronic metabolic disorder that has reached epidemic levels around the world.1 In China, there has been a sharp increase in diabetes prevalence in the past few decades, and currently 11.4 million people have diabetes.2 From both clinical and public health perspectives, there is a critical need to develop cost-effective strategies to prevent diabetes. Vitamin B12 is a coenzyme in the one-carbon metabolic pathway involved in the synthesis of methionine and pyrimidine and purine bases. Deficiencies in vitamin B12 and associated DNA damage and subsequent faulty repair are known to contribute to the development of vascular diseases, cancer, and some birth defects, and can lead to hyperhomocysteinemia. Often related to folic acid deficiency, vitamin B12 has been identified as a risk factor for both hypertension and atherosclerosis.3
To date, most studies on vitamin B12 and DM have been centered on vitamin B12 deficiency among existing patients with diabetes. The association between metformin use and low vitamin B12 levels has been supported by various levels of evidence.4 Because ileal vitamin B12 absorption is a calcium-dependent process, and metformin is known to have an effect on calcium-dependent membrane action, patients with type 2 diabetes usually developed a marked reduction in serum vitamin B12 while being treated with metformin.5 However, the risks and benefits of vitamin B12 on future risk of DM are not clear due to inconsistent results of previous studies. A cross-sectional study in a South Indian population showed that higher vitamin B12 levels decreased the risk of DM.6 Another longitudinal randomized control trial study showed no difference in the incidence of type 2 diabetes mellitus between the vitamin B12-supplemented group as compared with the non-supplemented control group.7 The current study addresses an important yet controversial topic of whether vitamin B12 is associated with DM.
This current study was motivated by the findings of the US National Health and Nutrition Examination Survey (NHANES)8 which showed that vitamin B12 levels in patients with DM without metformin were significantly higher than those in the general population. However, the NHANES is a cross-sectional study, and in order to address whether vitamin B12 levels that are higher than the optimal range are a risk factor for developing DM, a prospective cohort study would be required to assess the temporal and dose–response relationship.
In this report, we analyzed a total of 16 699 participants with hypertension from the China Stroke Primary Prevention Trial (CSPPT), with pertinent baseline data and a mean follow-up of 4.5 years. Our primary objective is to perform both cross-sectional and longitudinal analyses with the aim of determining whether the findings of the NHANES could be replicated in a Chinese population, and furthermore whether there is a prospective and dose–response association between baseline vitamin B12 levels and risk of new-onset DM. Among a subset of the sample (n=4366) with both baseline and exit vitamin B12 measurements, we further analyzed the relationship between the change in vitamin B12 levels and the change in fasting blood glucose (FBG) levels from baseline to the exit visit as the secondary objective.
Research design and methods
Participants and trial design
All participants provided written, informed consent. A total of 20 702 eligible participants, stratified by the methylenetetrahydrofolate reductase (MTHFR) C677T genotypes (CC, CT, or TT), were randomly assigned, in a 1:1 ratio, to one of two treatment groups: a daily oral dose of one tablet containing 10 mg enalapril and 0.8 mg folic acid (the enalapril-folic acid group), or a daily oral dose of one tablet containing 10 mg enalapril only (the enalapril group). Participants were engaged in follow-up visits every 3 months.
A detailed description and the primary results of the CSPPT have been reported elsewhere.9–11 Briefly, the CSPPT was a multicommunity, randomized, double-blind, controlled trial conducted between May 19, 2008 and August 24, 2013 in 32 communities in China. Eligible participants were men and women aged 45–75 years with hypertension, defined as seated, resting systolic blood pressure (SBP) ≥140 mm Hg or diastolic blood pressure (DBP) ≥90 mm Hg at both the screening and recruitment visit, or who were taking antihypertensive medication. The major exclusion criteria included history of physician-diagnosed stroke, myocardial infarction (MI), heart failure, postcoronary revascularization, or congenital heart disease. According to the CSPPT study protocol people who had long-term B-group vitamin supplementation were excluded, and other B-group vitamins should not be supplemented during the study period.
This report included 16 699 men and women with hypertension from the CSPPT with baseline vitamin B12 data and pertinent baseline and follow-up data on diabetes status and covariables. As illustrated in the flow chart (online supplementary figure S1), the final analyses excluded participants with missing values for baseline vitamin B12, baseline FBG, exit FBG and with any missing data on the follow-up questionnaire. We also randomly selected a subset of the population (n=4366) to detect changes in vitamin B12 at the exit visit (online supplementary table S1).
Supplemental material
Outcomes
Patients were classified as diabetic if they self-reported a physician diagnosis, or were using glucose-lowering medication, or when their FBG ≥7.0 mmol/L at baseline.12 New-onset diabetes was defined as a self-reported physician diagnosis, or use of glucose-lowering drugs during the follow-up period, or when FBG changed from <7.0 mmol/L at baseline to ≥7.0 mmol/L at the last study (exit) visit.
Covariables
Covariables included known or suspected factors associated with vitamin B12 and/or DM based on existing literature, including our own studies in the CSPPT, specifically age, sex, MTHFR gene C677T polymorphisms, SBP and DBP at baseline, mean SBP and DBP during the treatment period, body mass index (BMI), study center, serum concentrations of folate, total homocysteine (tHcy), total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), smoking status, alcohol consumption status, self-reported meat consumption and medication use. Information on meat consumption was self-reported at baseline using a simple abbreviated semiquantitative Food Frequency Questionnaire. Participants were asked to report how often, on average, they eat meat every week. Possible response categories included ‘never’, ‘1–2 times/week’, ‘3–5 times/week’ and ‘every day’. Vitamin B12 deficiency was defined as vitamin B12 <148.0 pmol/L.13
Laboratory assays
For biochemical analyses, 20 mL blood samples were collected between 7:00 and 9:00 after an overnight fast (at least 8 hours). Serum samples were separated, aliquoted and subsequently stored at –80°C until analysis. Plasma vitamin B12 at baseline and folate at baseline and the exit visit were measured using a chemiluminescent immunoassay at the commercial lab (New Industrial, Shenzhen, China). tHcy, fasting lipids and FBG at baseline and the exit visit were measured using automatic clinical analyzers (Beckman Coulter, California, USA) at the core lab of the National Clinical Research Center for Kidney Disease (Nanfang Hospital, Guangzhou, China).
Statistical analysis
Descriptive data are presented as mean (SD) or median values with IQR in parentheses or proportions, as appropriate, for population characteristics according to baseline vitamin B12 quartiles. The significance of differences in population characteristics between groups was computed using two-sample t-tests, signed-rank tests, or χ2 tests for continuous and categorical variables.
Logistic regression models were used to estimate the ORs and their 95% CIs of diabetes, given the exact onset of diabetes was not known and many new-onset DM cases were detected by fasting glucose levels at the exit visit. All analyses were conducted with adjustments for covariables. Finally, subgroup analyses were performed to evaluate possible effect modifications by the covariables on the association between vitamin B12 and DM, including sex (male vs female), age (<60 vs ≥60 years), MTHFR C677T polymorphism (CC vs CT vs TT), SBP (<160.0 vs ≥160.0 mm Hg), DBP (<90 vs ≥90 mm Hg), mean SBP during the treatment period (<140.0 vs ≥140.0 mm Hg), mean DBP during the treatment period (<90 vs ≥90 mm Hg), BMI (<25 vs ≥25 kg/m2), study center (Anqing vs Lianyungang), folate (<8 vs ≥8 ng/mL), tHcy (<12.5 vs ≥12.5 μmol/L), TC (<5.5 vs ≥5.5 mmol/L), TG (<1.5 vs ≥1.5 mmol/L), HDL-C (<1.3 vs ≥1.3 mmol/L) and treatment group (enalapril vs enalapril-folic acid). A two-tailed p<0.05 was considered significant in all analyses. All statistical analyses were performed using R software, V.3.6.0 (http://www.R-project.org/, accessed April 26, 2019).
Results
Study participants and baseline characteristics
Study participants had an average age of 60.0 years (SD 7.4), 6713 were male (40.2%) and 9986 were female (59.8%) (online supplementary table S2). Participants had an average vitamin B12 level of 295.9 pmol/L (SD 91.5), 257 (1.5%) participants had vitamin B12 deficiency, while 10 468 (63.3%) participants did not consume meat. The mean FBG level was 5.8 mmol/L (SD 1.7) at baseline, and the exit mean FBG level was 6.3 mmol/L (SD 2.0). At baseline, 1872 (11.2%) participants had DM, and at the exit visit there were 1589 (10.7%) cases of new-onset DM. When stratified by baseline vitamin B12 quartiles, FBG levels were the highest (6.0 mmol/L (SD 2.1)) in the fourth quartile (Q4). Table 1 shows that the average age and BMI of the participants in Q4 were lower than those of the other groups, but TC and TG levels were higher than the other quartiles.
Baseline and follow-up characteristics of the study participants by baseline B12 quartiles
Cross-sectional analysis on baseline vitamin B12 and DM
From the cross-sectional analysis, vitamin B12 was found to be positively associated with DM (OR=1.35, 95% CI 1.26 to 1.44, p<0.001) at baseline (table 2). After stratifying by vitamin B12 quartiles, participants in Q4 were found to have the highest risk (OR=1.68, 95% CI 1.43 to 1.98, p<0.001). Also, there was a positive association between vitamin B12 and FBG (β=0.14, 95% CI 0.11 to 0.17, p<0.001) (table 3). After stratifying by relevant covariables, we discovered interactions between sex, TC levels and vitamin B12 with baseline DM and FBG (online supplementary figure S2, online supplementary figure S3). No interaction was found between vitamin B12 and plasma folic acid or tHcy.
Cross-sectional and longitudinal association between baseline vitamin B12 levels and diabetes (DM) and new-onset DM
Cross-sectional and longitudinal association between baseline vitamin B12 and baseline FBG, exit FBG and change in FBG (ΔFBG)
Longitudinal analyses on baseline vitamin B12 and new-onset DM
Longitudinal analyses did not show an association between baseline vitamin B12 and new-onset DM (OR=0.97, 95% CI 0.90 to 1.04, p=0.346) (table 2), change in FBG (β=−0.01, 95% CI −0.04 to 0.02, p=0.602), or exit FBG (β=−0.01, 95% CI −0.04 to 0.02, p=0.602) after making additional adjustments for baseline FBG (table 3). After stratifying by relevant covariables, no interaction was found between vitamin B12 with new-onset DM, exit FBG or change in FBG (online supplementary figure S2, online supplementary figure S3).
Longitudinal analyses on change in vitamin B12 levels and change in FBG levels
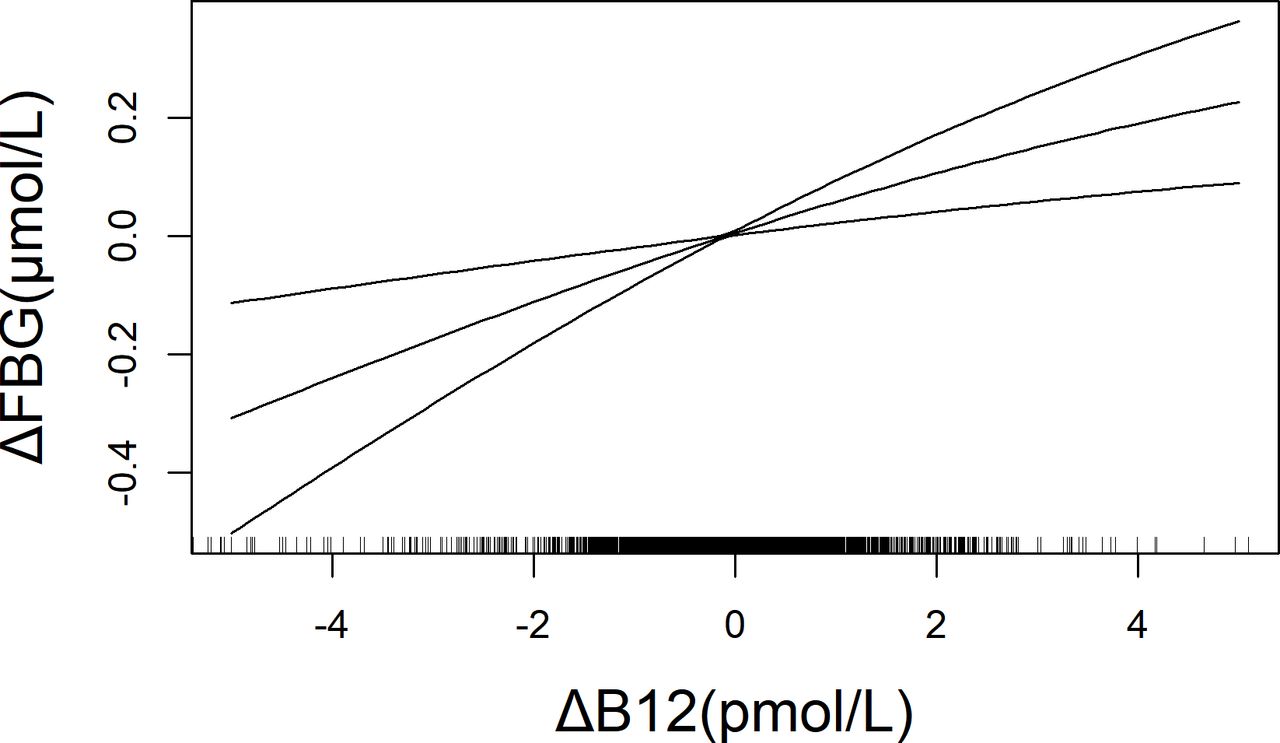
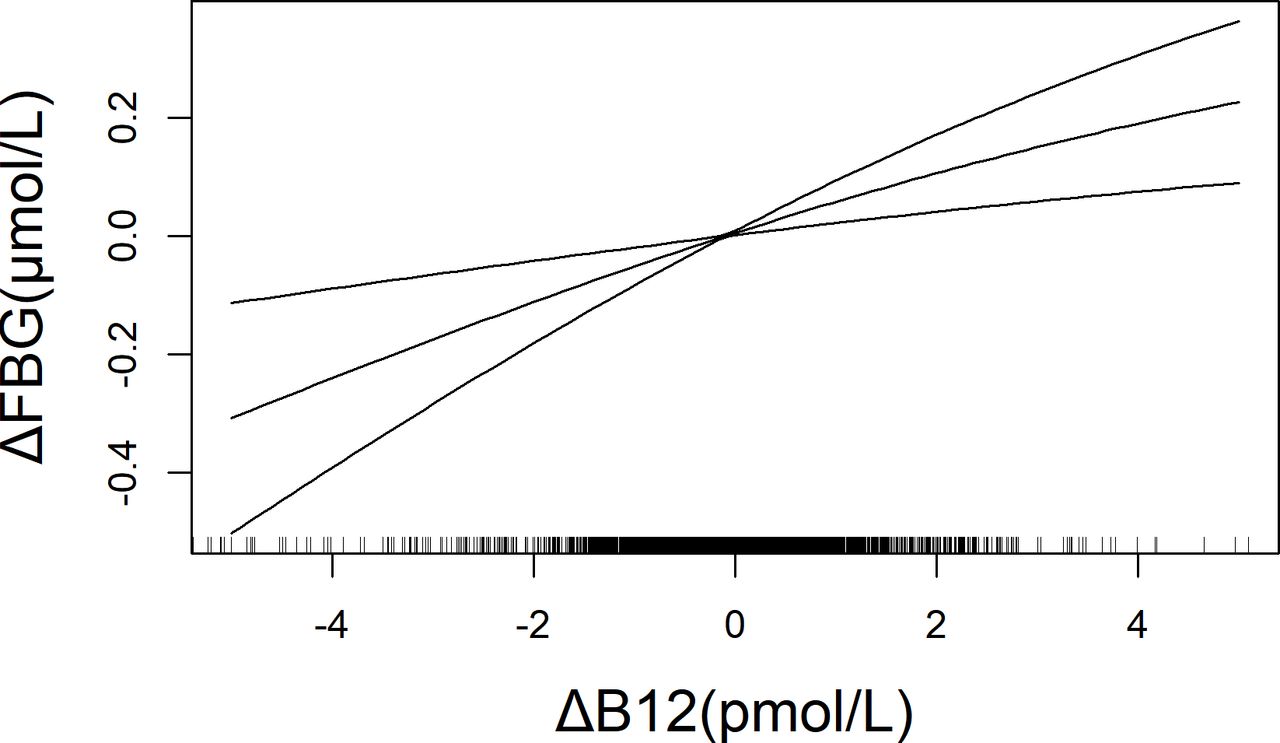
Among a subset of the sample (n=4366) with both baseline and exit vitamin B12 measurements, we further analyzed the relationship between change in vitamin B12 levels and change in FBG levels from the baseline to the exit visit. We found a dose–response relationship between change in vitamin B12 and change in FBG levels (table 4, figure 1).
Longitudinal analyses on change in vitamin B12 (ΔB12) and change in’ FBG (ΔFBG) from baseline to exit visit*
{kind=link}
Multivariable-adjusted smoothing curves of change in vitamin B12 and change in FBG in a subsample that included a total of 4366 subjects with both baseline and exit FBG and vitamin B12 measurements. Adjusted for age, sex, MTHFR gene C677T polymorphisms, SBP and DBP at baseline, mean SBP and DBP during the treatment period, body mass index, study center, baseline serum concentrations of folate, homocysteine, FBG, vitamin B12, total cholesterol, triglycerides, and high-density lipoprotein cholesterol, treatment group, smoking status, and alcohol consumption status. DBP, diastolic blood pressure; FBG, fasting blood glucose; MTHFR, methylenetetrahydrofolate reductase; SBP, systolic blood pressure.
Discussion
This is the first time that the relationship between vitamin B12 and DM has been explored in a Chinese population of patients with hypertension via both cross-sectional and longitudinal analyses. We confirmed the findings of the NHANES, showing a cross-sectional positive association between vitamin B12 and DM at baseline in this Chinese population. Furthermore, our longitudinal analyses demonstrated that there was no association between baseline vitamin B12 levels and new-onset DM risk. Our study has contributed new insights on the vitamin B12 and DM association and has helped to explain inconsistent findings in previous studies.
Vitamin B12 and DM association depends on population characteristics
Most previous studies on the association of vitamin B12 and DM were centered on vitamin B12 deficiency among existing patients with DM with the use of metformin. The association between metformin use and low vitamin B12 levels has been supported by various levels of evidence.4 Most of those studies were conducted in older populations, where vitamin B12 deficiency is more likely.8 In contrast, our study was conducted in a Chinese population of patients with hypertension who were relatively young (45–75 years at baseline), mostly free from DM at baseline, and mostly vitamin B12 sufficient. Only 6.9% of the study participants with DM reported using metformin (online supplementary figure S4).
Vitamin B12 and DM association depends on the study design and type of analyses
In a Mendelian randomization study, Moen et al14 found that vitamin B12 may have a causal effect on fasting glucose and one potential mechanism could be an effect of vitamin B12 on cell cycle and proliferation of pancreatic β cells, resulting in improved insulin secretion among individuals with higher vitamin B12 concentrations. However, in other cross-sectional analyses, Jayashri et al6 found that the levels of vitamin B12 decreased with increasing severity of glucose tolerance. Margalit et al15 found no significant difference in blood sugar between the vitamin B12-deficient group and the non-deficient group. In longitudinal analyses and randomized trials, Looker et al16 found that vitamin B12 was positively associated with all-cause mortality and death from diabetes/nephropathy. Song et al7 found that daily supplementation with folic acid and vitamins B6 and B12 did not reduce the risk of developing type 2 diabetes among women at high risk for cardiovascular diseases (CVD). Kwok et al17 found that vitamin B12 supplementation did not prevent cognitive decline in older patients with diabetes with borderline vitamin B12 status. In a systematic review, Rafnsson et al18 found that current data do not support vitamin B12 supplementation in reducing the risk of cardiovascular diseases or diabetes.
Our study was the first to perform and report findings from both cross-sectional and longitudinal analyses in the same population. In the cross-sectional analysis, we found an independent, positive association between baseline vitamin B12 levels and DM and FBG. These results persisted even after we adjusted for relevant covariables. This finding is consistent with the NHANES study.8 In the longitudinal analyses, we did not find any association between baseline vitamin B12 and new-onset DM risk. This finding is consistent with the Women’s Antioxidant and Folic Acid Cardiovascular Study, where women aged ≥40 years with a history of cardiovascular disease, who were free of DM at baseline, were supplemented with either a combination pill consisting of folic acid, pyridoxine and vitamin B12, or a placebo. After a median follow-up of 7.3 years, no difference in incident type 2 diabetes mellitus was found between the two groups.7 Another longitudinal study19 in Japan also reported similar null results. Taken together, our longitudinal analyses and that of others did not support an association between vitamin B12 and new-onset DM. These findings underscore that cross-sectional associations need to be confirmed by prospective studies and clinical trials, because the former is more likely to be subject to many drawbacks, including reverse causality.
Clinical implications of findings
The role of vitamin B12 in DM varied by patient characteristics. Most previous studies have shown that vitamin B12 supplementation is necessary in elderly patients with diabetes with low vitamin B12 levels or in patients with diabetes with long-term metformin use.8 17 20 Our study, along with other longitudinal studies, however, does not support the routine use of vitamin B12 supplementation to reduce the risk of new-onset DM18 in relatively young patients with no evidence of vitamin B12 deficiency. Moreover, a meta-analysis by Valdés-Ramos et al21 indicated no recommendation for the use of vitamin supplements in patients with type 2 diabetes mellitus. Of note, the research of Looker et al16 showed that vitamin B12 was positively associated with all-cause mortality and death from diabetes/nephropathy, and previous data also indicated that elevated serum vitamin B12 levels are a predictive factor for mortality in elderly patients with cancer.22 Salles et al23 and Hemmersbach-Miller et al24 reported that higher vitamin B12 levels might also be a marker to assess a higher risk of mortality in elderly patients. Vitamin B12 can also accelerate decline in renal function and increase the risk of cardiovascular events in patients with impaired renal function.25 26 Zeitlin et al27 also suggest that for elderly people, vitamin B12 supplementation should not be routinely provided unless there are clear indications for doing so (a deficiency state), and then to only replace enough vitamin B12 to correct the deficiency. Through our research and analysis, we found that vitamin B12 may still have a correlation with blood glucose or DM, and the disappearance of this correlation in the longitudinal analysis may be due to the relative changes in the observation age, the decrease in vitamin B12 levels and the increase in FBG levels over time. Therefore, the relationship between the changes in indicators needs to be observed to reflect real results. We found that the change in vitamin B12 levels and the change in FBG levels showed a positive vitamin B12–FBG association in the subsample. In addition, we repeated the previous analysis with this subsample and found the results were consistent with those of the previous analysis (online supplementary table S3).
The present study had some limitations. First, this study focused on Chinese adults with hypertension, so the generalizability of the results to other populations remains to be determined. Second, new-onset DM was not a primary outcome or a prespecified outcome of the CSPPT. We did not obtain FBG measurements at the scheduled follow-up visits, nor did we measure hemoglobin A1c or perform glucose tolerance tests at baseline or during the follow-up visits. Therefore, it is possible that we have underestimated the incidence of new-onset DM in the CSPPT. Nevertheless, we believe that any potential underestimation of new-onset DM should be non-differential, and therefore should not significantly affect the results. Finally, we only measured vitamin B12 levels on a small subset (n=4366) of the population at the exit visit and were unable to examine vitamin B12 dynamics during the follow-up period of the CSPPT.
Conclusion
Among a population of adults with hypertension in China without a history of stroke or MI, who were mostly vitamin B12-sufficient, there was a dose–response association of vitamin B12 levels with the risk of DM based on cross-sectional analyses at baseline. There was no prospective relationship between baseline vitamin B12 and new-onset DM in the longitudinal analyses. However, in a subsample, a positive vitamin B12–FBG association was shown by the change in vitamin B12 levels and the change in FBG levels. This result indicates that there may be a potential correlation between B12 and diabetes. Our findings illustrate a clear discrepancy in results from the cross-sectional and longitudinal analyses even from the same study population, and underscore the need to consider both baseline and longitudinal changes between vitamin B12 and FBG in order to better elucidate the role of vitamin B12 in the development of diabetes. If further studies confirm such findings, this will have an important impact on clinical and public health.
References
Footnotes
Contributors XX, YH and HZ critically revised the protocol for research design. LL, XH, YS, TL, ZZ, ZW, PC, and GT were responsible for implementation on-site. LL, XH and CL performed the statistical analyses. LL and XH drafted the manuscript. XW, PAZ, YY, WL, JL, YZ, YL, XQ and BW developed the methodological approach. All authors contributed to the conception and design and approved the final version of the manuscript.
Funding The China Stroke Primary Prevention Trial (CSPPT) was jointly supported by Shenzhen AUSA Pharmed (Shenzhen, China) and national, provincial and private funding, including from the Major State Basic Research Development Program of China (973 Program; grant no. 2102 CB517703); the National Science and Technology Major Projects Specialized for ‘Innovation and Development of Major New Drugs’ during the 12th Five-year Plan Period: the China Stroke Primary Prevention Trial (grant no. zx09101105); a Clinical Center grant (no. zx09401013); the Projects of the National Natural Science Foundation of China (grant no. 81473052, 81441091, and 81402735); the National Clinical Research Center for Kidney Disease, Nanfang Hospital, Nanfang Medical University, Guangzhou, China; the State Key Laboratory for Organ Failure Research, Nanfang Hospital; and research grants from the Department of Development and Reform, Shenzhen Municipal Government (grant no. SFG 20201744).
Disclaimer The funding organizations and/or sponsor participated in the study design, but had no role in the conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Competing interests XX reports grants from the National Key Research and Development Program (2016YFE0205400, 2018ZX09739010, 2018ZX09301034003), the Science and Technology Planning Project of Guangzhou, China (201707020010), the Science, Technology and Innovation Committee of Shenzhen (JSGG20170412155639040, GJHS20170314114526143, JSGG20180703155802047), and the Economic, Trade and Information Commission of Shenzhen Municipality (20170505161556110, 20170505160926390). YL reports grants from the President Foundation of Nanfang Hospital, Southern Medical University (2017C007, 2018Z009). XQ reports grants from the National Natural Science Foundation of China (81730019, 81973133) and Outstanding Youths Development Scheme of Nanfang Hospital, Southern Medical University (2017J009). HG reports grants from the 111 Project from the Education Ministry of China (B18053). XH reports grants from the National Natural Science Foundation of China (81960074, 81500233), Jiangxi Outstanding Person Foundation (20192BCBL23024), and major projects of the Science and Technology Department, Jiangxi (20171BAB205008).
Patient consent for publication Not required.
Ethics approval The parent study (the CSPPT) was approved by the Ethics Committee of the Institute of Biomedicine, Anhui Medical University, Hefei, China (Federal-wide Assurance Number: FWA00001263).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.