Article Text

Abstract
Objective To determine glycemic control in adult patients with type 2 diabetes receiving antidiabetic therapy as part of routine healthcare in India.
Research design and methods This was a retrospective analysis of cross-sectional data of patients with type 2 diabetes receiving oral hypoglycemic agents (OHAs) with or without insulin between 2015 and 2017. We assessed proportion of patients with uncontrolled glycemia and performed logistic regression to evaluate its association with various risk factors and microvascular complications.
Results A total of 55 639 eligible records were identified; mean age of patients was 54.31 (±11.11) years. One-third of the study population had microvascular complications, predominantly neuropathy. Nearly 76.6% of patients had uncontrolled glycated hemoglobin (HbA1c) ≥7% (53 mmol/mol); 62% of these patients had HbA1c between 7% and 8% (53–64 mmol/mol). Glycemic control from combination of OHAs with or without insulin varied between 14.2% and 24.8%. In multivariate analysis, factors statistically associated with uncontrolled glycemia were obesity (OR: 1.15), hypertension (stage I OR: 1.65 and stage II OR: 2.73) and diabetes duration >5 years (OR: 1.19) (p<0.001). Similarly, the odds of having any microvascular complication increased with duration of diabetes (past 1–2 years, OR: 1.67; 2–5 years, OR: 2.53; >5 years, OR: 4.01; p<0.0001), hypertension (stage I, OR: 1.18 and stage II, OR: 1.34; p<0.05) and uncontrolled HbA1c (OR: 1.28; p<0.0001).
Conclusions Indian population with type 2 diabetes has a high burden (76.6%) of poor glycemic control. This study highlights the need for early implementation of optimum diabetes pharmacotherapy to maintain recommended glycemic control, thereby reducing burden of microvascular complications.
- A1C
- type 2 diabetes
- body mass index
- hypertension
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of the study
What is already known about this subject?
India has emerged as the diabetes capital due to an interplay of modifiable and non-modifiable risk factors, but faces crucial challenges like pockets of underserved population both in urban and rural areas, lack of medical insurance, inadequate data reporting, clinical inertia and poor drug adherence—all of which are required for achieving glycemic targets.
What are the new findings?
This study confirms the real burden of uncontrolled type 2 diabetes with a fairly large urban population across different geographies in India, concomitant with a high prevalence of microvascular complications and comorbidities like obesity and hypertension.
Usage of newer antidiabetic class of drugs is increasing in our population; however, their impact on glycemic control could not be studied due to cross-sectional design of the study.
How might these results change the focus of research or clinical practice?
This study highlights the need for early implementation of optimum diabetes pharmacotherapy to maintain recommended glycemic control, thereby reducing burden of microvascular complications.
Introduction
The pandemic of diabetes mellitus has affected an estimated 451 million people worldwide in 2017 and is projected to affect 693 million people by 2045.1 India has emerged as the diabetes capital in the Southeast Asian region having the highest number of people with diabetes (74 million), with an age-adjusted comparative prevalence of 9.8% in the age group of 18–99 years and premature mortality of 50.7% (20–79 years).2 The overall prevalence of diabetes in 15 Indian states sampled in the Indian Council of Medical Research-India Diabetes (ICMR-INDIAB) population-based cross-sectional study was 7.3%.3 The epidemiological transition in India, in synergy with aging population and comorbid conditions such as obesity and hypertension, has played a catalyst in driving the diabetes epidemic in rural areas (5.2%) alongside the urban ones (11.2%).3
Indians have a ‘thin‐fat’ phenotype (anthropometrically thin, but metabolically obese) characterized by low lean body mass and high subcutaneous fat, together with the triad of metabolic derangements (glucose and lipid dysregulation, abdominal obesity, and elevated blood pressure). This phenotype accentuates susceptibility for insulin resistance and development of type 2 diabetes.4 Indians have a tendency for earlier onset of type 2 diabetes, leading to an accelerated risk of developing microvascular (neuropathy, nephropathy, and retinopathy) and macrovascular complications (cardiovascular, peripheral vascular, and cerebrovascular diseases).5 However, diabetes is often diagnosed only after the disease has exacerbated to an advanced stage with microvascular complications.6 The landmark UK Prospective Diabetes Study demonstrated that a 1% reduction in glycated hemoglobin (HbA1c) by intensive hypoglycemic therapy is associated with a 37% decrease in risk for microvascular complications.7
Most guidelines consider HbA1c ≤7% (53 mmol/mol) as the general target of glucose control for optimum diabetes management.8–11 The Research Society for the Study of Diabetes in India has released comprehensive clinical practice recommendations for the management of type 2 diabetes, which are derived from the International Diabetes Federation Global Guideline for type 2 diabetes.12 A patient-centered approach is essential for achieving glycemic targets after considering age, body mass index (BMI), chronic kidney disease, duration of diabetes, established cardiovascular disease, financial condition, and glycemic status.12 Early initiation of a combination therapy, without undue delay of insulin, can be instrumental in achieving better glycemic targets, impeding clinical inertia, and ultimately attenuating the development of complications.13
The management of type 2 diabetes poses a unique and complex health challenge in India, where the burden is higher than that in developed countries but may be masked by inadequate reporting and substantially lower number of diabetes registries. Clinical inertia, poor drug adherence, and low disease awareness are crucial challenges for achieving glycemic targets, especially in the real-world clinical setting.12 14 Real-world evidence can help bridge the evidence gap by providing better insights for prescribing patterns, drug adherence, comorbidities, and effects of switching or adjusting medications in the real world.15 In 2006, the ICMR had established a multicenter clinic-based registry of diabetes with young age at onset for individuals <25 years.16 However, real-world data on glycemic control among adult patients from India are scarce. Hence, we conducted a large pan-India cross-sectional registry study to determine glycemic control among adult patients with type 2 diabetes mellitus, their ongoing antidiabetic therapy, and associated microvascular complications.
Research design and methodology
This article presents data on glycemic control from the TIGHT (The Investigation of Glycosylated Hemoglobin on Therapy in Indian diabetics) study. This was a retrospective analysis of cross-sectional data collected from over 3196 urban healthcare facilities across 26 states and union territories between 2015 and 2017. Private healthcare facilities were selected representing the north, south, east, west, and central regions. Retrospective data were collected from anonymized patient records; hence, the study was exempted from ethical clearance. Enrolled population included patients with type 2 diabetes mellitus of either gender who were on treatment with one or more oral hypoglycemic agents (OHAs) or in combination with insulin. Data of patients with type 1 diabetes and those with missing values were excluded. Protocol-defined data were transcribed on a case record form after ensuring accuracy and completeness.
The study was primarily designed to determine the proportion of patients with type 2 diabetes across the country with or without glycemic control after receiving antidiabetic treatment. Demographic and clinical factors including microvascular complications and therapeutic options associated with optimal glycemic control were also explored. The optimal glycemic control in non-pregnant adults was defined as HbA1c <7% (53 mmol/mol); uncontrolled diabetes HbA1c ≥7% (53 mmol/mol); fasting blood glucose (FBG) ≤130 mg/dL (7.2 mmol/L), FBG >130 mg/dL (7.2 mmol/L); and post-prandial blood glucose (PPG) <180 mg/dL (10.0 mmol/L), PPG ≥180 mg/dL (10.0 mmol/L) according to the Standards of Medical Care in Diabetes by the American Diabetes Association (ADA) 2018.8 Blood pressure (mm Hg) was categorized as normal (systolic blood pressure (SBP) <120 mm Hg and diastolic blood pressure (DBP) <80 mm Hg), prehypertension (SBP=120–139 mm Hg or DBP=80–89 mm Hg), stage I hypertension (SBP=140–159 mm Hg or DBP=90–99 mm Hg), and stage II hypertension (SBP ≥160 mm Hg or DBP ≥100 mm Hg).17 BMI was classified according to the consensus statement for diagnosis of obesity, abdominal obesity, and the metabolic syndrome for Asian Indians by Misra et al: normal BMI: 18–22.9 kg/m2, overweight 23–24.9 kg/m2, obese: >25 kg/m2.18 We also examined the associations among diabetes duration, glycemic control, and microvascular complications. Diabetes duration (based on treatment period) was categorized as follows: recently diagnosed, <1 year since diagnosis, diagnosed in past 1–2 years, diagnosed in past 2–5 years, and diagnosed >5 years ago. The microvascular complications were reported as diabetic neuropathy, nephropathy, and retinopathy. For subgroup analysis, patients were categorized into one of two cohorts (<5 years and ≥5 years) based on the duration of diabetes. The patients were then further classified into two cohorts based on the number of antidiabetic medications (<3 therapies and ≥3 therapies) and glycemic control (HbA1c <7%; 53 mmol/mol and HbA1c ≥7%; ≥53 mmol/mol). The following parameters were assessed for each patient cohort: age, gender, BMI, hypertension, FBG, PPG, and microvascular complications.
Data collection and statistical analysis
Data collection included demographics, anthropometric measures, duration of type 2 diabetes, antidiabetes therapy, vital signs, laboratory results (HbA1c, fasting and postprandial glucose levels, and urine glucose level), comorbidities, microvascular complications, and concomitant medications. Summary statistics for quantitative variables included the number of observations (n), mean, SD, minimum, maximum, and median. Qualitative variables are presented with absolute and relative frequencies. A bivariate analysis between uncontrolled and controlled diabetes for all covariates and outcomes was performed (χ2 test for categorical variables). Univariate and multivariate logistic regression were performed to evaluate the association among uncontrolled glycemic status, microvascular complications, and other factors. Statistical analyses were performed using SAS V.9.4, and p-value <0.05 was considered statistically significant.
Results
Demographic and clinical profile
A total of 55 639 eligible patient records aged ≥18 years were identified between 2015 and 2017. Most patients (53.2%) were <55 years, and the mean (±SD) age of patients was 54.31 (±11.11) years. Males accounted for 54.1% of the study population. The mean BMI of patients was 26.37 (±3.31) kg/m2; it was similar across gender (males: 26.38 (±3.26); females: 26.36 (±3.37)). Comparable proportion of men and women were obese and overweight (males: 67.8% and 20.4%; females: 66.7% and 20.4%), respectively. Table 1 summarizes the demographic and clinical characteristics of patients having controlled or uncontrolled glycemic status. Two-thirds of patients reported having diabetes for a duration of >2 years (2–5 years: 29.9% and >5 years: 37.6%). About 67.1% of patients had prehypertension, followed by stage I (25%) and stage II hypertension (3%) (table 1). Of the total study population, 33 114 (59.5%) patients were on statin therapy.
Characteristics of patients with type 2 diabetes having controlled or uncontrolled glycemia
Glycemic control
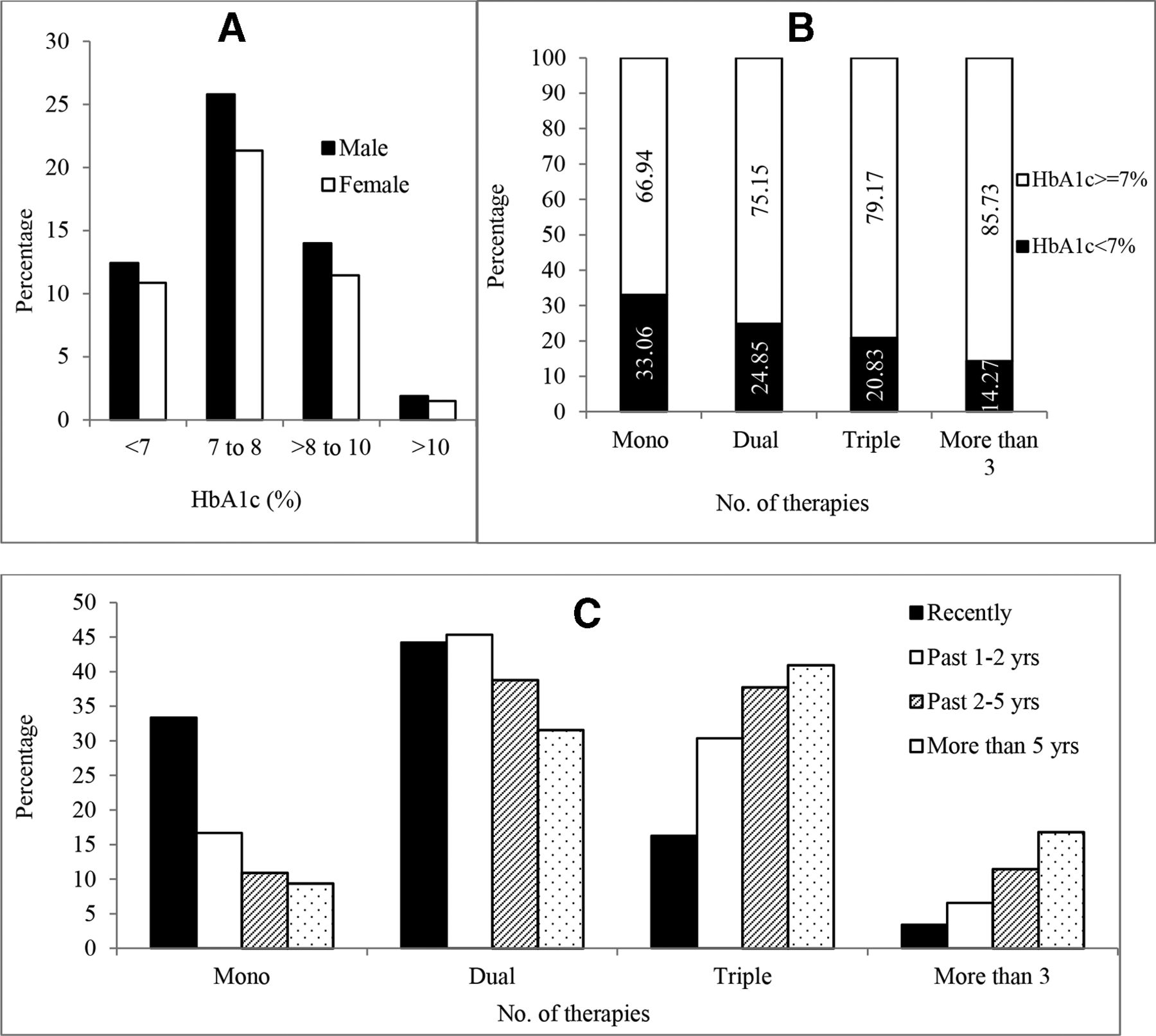
The mean±SD HbA1c, FBG, and PPG values were 7.7% (61 mmol/mol)±1.09, 126.8 mg/dL (7.03 mmol/L)±19.02, and 198.27 mg/dL (11.0 mmol/L)±43.51, respectively. Nearly three-fourths (76.6%) of patients had uncontrolled HbA1c ≥7% (≥53 mmol/mol). Of patients with uncontrolled diabetes, a substantial proportion (62%) had HbA1c between 7% and 8% (53–64 mmol/mol), 33.6% had HbA1c between 8% and 10% (64–86 mmol/mol), while a minor proportion (4.4%) had HbA1c >10% (86 mmol/mol) (figure 1A). Overall, 42.4% of patients had FBG >130 mg/dL (7.2 mmol/L), of which 87.0% had HbA1c ≥7% (53 mmol/mol). However, among patients FBG <130 mg/dL (7.2 mmol/L) (57.6%), 68.9% had HbA1c ≥7% (53 mmol/mol). Similarly, 62.9% of patients had PPG >180 mg/dL (10.0 mmol/L), of which 85.7% had HbA1c ≥7% (>53 mmol/mol). Among patients with PPG <180 mg/dL (10.0 mmol/L) (37.1%), 61.0% had HbA1c ≥7% (>53 mmol/mol). The glycemic status had profound variations across the country, with a higher proportion of patients with type 2 diabetes having uncontrolled glycemia in Southern region (online supplemental figure 1). Of patients with obesity, 77.6% had uncontrolled HbA1c and of patients with hypertension, 81% had HbA1c ≥7% (≥53 mmol/mol). Of patients with diabetes duration >2 years, HbA1c was under control in only 21.8% (2–5 years: 22.7% and >5 years: 21.1%). The effect of comorbidities like obesity and hypertension on HbA1c levels was exemplified in logistic regression for uncontrolled glycemia. The covariates in multivariate logistic regression included age, gender, BMI, blood pressure, disease duration, statin, number of therapies and microvascular complication. In multivariate analysis, obesity, hypertension, diabetes duration (≥2 years), and number of therapies were statistically associated with uncontrolled glycemia (table 2).
Supplemental material
Logistic regression to determine factors associated with any microvascular complications and uncontrolled diabetes

(A) Percentage of patients with glycated hemoglobin (HbA1c) categories showing glycemic control status of study population grouped by gender. (B) HbA1c status and number of hypoglycemic therapies used (dual, triple, and more than three therapies include patients with or without insulin). (C) Percentage of patients with different duration of diabetes grouped by number of hypoglycemic therapies.
Obese patients had significantly higher odds with OR of 1.15 (95% CI 1.07 to 1.23) for uncontrolled glycemia compared with patients having a normal BMI (p<0.0001). The OR for uncontrolled diabetes status increased from stage I (OR=1.65) to stage II (OR=2.73) hypertension (p<0.0001). The multivariate analysis also demonstrated a significant association of uncontrolled glycemia with increasing duration of type 2 diabetes compared with recently diagnosed diabetes: past 2–5 years, OR 1.15 (95% CI 1.06 to 1.25); >5 years, OR 1.19 (95% CI 1.10 to 1.29) (table 2). The number of diabetic therapies was also significantly associated with uncontrolled glycemia (table 2).
Antidiabetic therapy
Most of the patients (73%) were taking dual or triple therapy, followed by monotherapy (14%), and 12% patients were taking more than three OHAs. Insulin use was reported among 17.2% of overall patients. Of the OHAs, 83.1% were taking metformin as monotherapy or combination therapy. Multiple therapies comprised sulfonylurea + metformin pill (60%) and combinations of different drugs including gliptins (53.1%), alpha-glucosidase inhibitors (15.5%), and thiazolidinediones 10%. Most patients (86.6%) diagnosed within 2 years were on metformin therapy either alone or as combination in accordance with the recent guidelines. The use of DPP-4 (dipeptidyl peptidase-4) inhibitor drugs as combination therapy increased from 47% in 2015 to about 60% in 2017. In our study population, usage of sodium–glucose cotransporter 2 (SGLT2) inhibitors as part of combination therapy was reported in about 10% of patients in the year 2017 (only 4.3% patients among the total population were under therapy). About 14% of patients were on monotherapy, while 85% were taking combination therapy. Of patients taking monotherapy, 33% had good glycemic control as compared with 21.7% among patients on combination therapies (figure 1B). Overall, the range of glycemic control for different combinations of OHAs with or without insulin varied between 14.2% and 24.8%. Irrespective of diabetes duration, patients on three or more OHAs and uncontrolled HbA1c levels had greater proportion of any microvascular complications.
Microvascular complications
About 35.7% of the patients had at least one microvascular complication; the proportion was higher for neuropathy (26.9%), followed by nephropathy (8.6%) and retinopathy (7.1%); and 15.4% patients had two or more complications. Overall, 80.4% of patients with any microvascular complication had uncontrolled diabetes status (table 1). The proportion of patients with microvascular complications progressively increased with duration of diabetes, especially neuropathy showing a steep rise compared with nephropathy and retinopathy (figure 2).

{kind=link}
{kind=link}
Duration of diabetes and various microvascular complications.
In the univariate analysis, older age (>65 years), male gender, obesity, hypertension, longer diabetes duration, and poor HbA1c control were predominant factors associated with increased risk of any microvascular complication (p<0.001) (table 2). The multivariate analysis demonstrated increasing odds of having any microvascular complication with longer duration of type 2 diabetes compared with recently diagnosed diabetes (past 1–2 years, OR 1.67 (95% CI 1.52 to 1.84); past 2–5 years, OR 2.53 (95% CI 2.31 to 2.78); >5 years, OR 4.01 (95% CI 3.66 to 4.39)). Furthermore, patients with hypertension (stage I OR=1.18 and stage II OR=1.34; p<0.05) and uncontrolled HbA1c (OR=1.28, p<0.0001) had significantly increased risk of any microvascular complication (table 2). Additionally, the multivariate analysis assessing risk factors specifically for neuropathy, nephropathy, and retinopathy showed that the odds were significantly higher among patients with uncontrolled HbA1c; neuropathy (OR=1.15), nephropathy (OR=1.38), and retinopathy (OR=1.47) (p<0.0001) (online supplemental table S1).
Discussion
This nationally representative cross-sectional study assessed the glycemic control in a very large urban sample of Indian adults with type 2 diabetes between 2015 and 2017 and explored the patterns of antidiabetic medication use. Our study results demonstrate the real-world burden of uncontrolled diabetes in India with only 23.4% of the study population reporting a good glycemic control (HbA1c <7%; 53 mmol/mol) with mean HbA1c of 7.7%±1.09. Similar results for glycemic control (HbA1c <7%; 53 mmol/mol) were reported in recent studies from Kerala (28.3%) and a registry database from 26 states across India (23.4%).19 20 The multicentric ICMR-INDIAB phase I study (N=480) reported a higher (31%) proportion of patients with glycemic control, with mean HbA1c of 9.1% (76 mmol/mol).21 Interestingly, 25.3% of patients from the ICMR-INDIAB study had HbA1c >10% compared with 4.4% in our study.21 This variation can be attributed to the fact that the ICMR-INDIAB study determined glycemic control among self-reported patients with diabetes.
Our study results show obesity, longer duration of diabetes, hypertension, and number of therapies to be significantly associated with poor glycemic control. Obesity and hypertension are well-established comorbidities for diabetes; a meta-analysis of observational studies from India showed a significant association between obesity and diabetes (pooled OR=1.14, 95% CI 1.04 to 1.24).22 Our study results showed that glycemic control becomes more difficult with increasing duration of diabetes even with the use of combination therapies, probably due to the progressive nature of diabetes. This is consistent with results from a retrospective study in China that reported >4 years of diabetes duration was associated with higher odds (OR=5.98, 95% CI 4.09 to 8.75) of poor glycemic control.23 The association between poor glycemic control and multiple therapies with or without insulin in our study is likely due to longer duration and disease severity. This can also be a reflection of inadequate drug adherence or clinical inertia. Furthermore, a study from India has reported a poor frequency of HbA1c monitoring among patients with diabetes.21 Self-monitoring of blood glucose level and enhancing medication adherence can be instrumental in meaningful improvements in HbA1c control.24 25 Additionally, the quality of diabetes management in India varies considerably with the awareness level, attitude, and perception of physicians on diabetes care.26
As a well-known consequence, this study also reports association of uncontrolled glycemia with the development of any microvascular complication. Nearly one-third of the population (35.7%) had any microvascular complication, predominantly neuropathy (26.9%), followed by nephropathy (8.6%) and retinopathy (7.1%). Previous studies from India have reported the prevalence of retinopathy (10.4%–32.5%), neuropathy (14.7%–29.2%), and nephropathy (6.2%–30.2 %) across healthcare facilities in north and south regions.27–30 The population-based Chennai Urban Rural Epidemiology Study (CURES) reported a comparable prevalence of neuropathy (25.7%) and nephropathy (5.1%); however, prevalence of retinopathy (17.5%) was much higher.31 The CURES further identified age, HbA1c, duration of diabetes, and serum triglycerides as major risk factors for the three microvascular complications. These findings are in line with the risk factors identified in our study. Stringent glycemic control remains crucial for the prevention of long-term microvascular complications. A meta-analysis from randomized controlled trials over 5 years reported that intensive glucose control compared with less intensive glucose control reduced relative risk by 20% for microvascular kidney events (HR 0.80, p<0.0001) and by 13% for eye events (HR=0.87, p=0.04), but not for nerve events (HR=0.98, p=0.68).32 Additionally, in people with diabetes, early intensive glucose control therapy not only lowers blood glucose levels but also reduces blood pressure, cholesterol, and its atherogenic subfractions.
Most patients in our study (86%) were consuming dual or multiple antidiabetic drugs, which increased with the disease duration (figure 1C). Prescription of combination therapy with metformin and newer OHAs including SGLT2 inhibitors and gliptins increased over the years. For the optimum management of type 2 diabetes, a proactive approach is recommended with individualized and early consideration of combination therapy. However, in India the stepwise approach of sequential addition of other OHAs to metformin monotherapy is often delayed.33 This results in a cascade of suboptimal glycemic control and increases the risk of microvascular and macrovascular complications. A meta-analysis demonstrated that early combination therapy with metformin compared with metformin alone leads to increase in the number of patients achieving HbA1c goal of <7%; <53 mmol/mol (relative risk 1.40).34 Early insulin initiation and/or intensification among patients with inadequately controlled type 2 diabetes can also be pivotal to achieve glycemic control.35 The consensus report by the ADA and the European Association for the Study of Diabetes 2018 recommend using SGLT2 inhibitors or GLP-1 (glucagon-like peptide) receptor agonists for patients with diabetes having comorbidities such as chronic kidney disease or clinical heart failure, alongside consistent efforts to improve diet and exercise.36
Limitations of the study include its cross-sectional and retrospective design because of which a causal relationship between glycemic control over the course of antidiabetic therapy and development of microvascular complications could not be established. Another challenge was missing data on macrovascular complications, which made it difficult to differentiate them from comorbidities if not distinctly documented in the medical records. Additionally, it was difficult to ascertain any coronary risk from the available data on statin therapy because of lack of information on dyslipidemia control. Data on anemia were not collected; however, the patients were from private set-up and so were less likely to have anemia.
Despite the above limitations, as one of the largest real-world study on glycemic control in India, our study highlights the need for early implementation of rigorous and optimum management of diabetes to mitigate the clinical and economic burden of managing microvascular complications. Thus, the challenge of early detection, screening, and awareness will always persist, what is essential is to achieve a target glycemic control in a reasonable time frame.
Conclusions
We performed a large real-world study to determine the levels of glycemic control among patients with type 2 diabetes in India. Our study results show a high burden of uncontrolled diabetes with three-fourths of 55 639 patients (76.6%) having a poor glycemic control (HbA1c ≥7%; 53 mmol/mol). Studies like the population-based ICMR-INDIAB study have reported similar levels of glycemic control among patients with type 2 diabetes across India. Nearly one-third of our study population had microvascular complications, predominantly neuropathy. The overall usage of newer OHAs including SGLT2 inhibitors and gliptins in combination therapy increased over the years. This large real-world study highlights the need for early implementation of optimum diabetes pharmacotherapy to maintain recommended glycemic control, thereby reducing burden of microvascular complications. Enhanced awareness among patients and providers, curbing clinical inertia, individualized patient-centered therapy, together with optimal care of comorbidities like hypertension and dyslipidemia remain the mainstay of reaching glycemic targets.
Research questions
Can early implementation of optimum combination therapy in type 2 diabetes, including the feasibility of using newer drugs like the GLP-1 agonists and sodium–glucose cotransporter 2 (SGLT2) inhibitors reduce the burden of uncontrolled glycemia and subsequent microvascular complications?
Explore the utility and cost-effectiveness of newer therapies like SGLT2 inhibitors in the Indian context for reducing the incidence of chronic kidney disease and heart failure as complications of long-standing diabetes?
Determine whether efforts to reduce the burden of type 2 diabetes such as primordial and primary prevention prove to be more effective in Indian context rather than relying on medical therapy?
Supplemental material
Acknowledgments
The authors thank all the physicians and doctors across India who kindly agreed to participate in the TIGHT study and extended their support for data collection (details of all the doctors are provided in the appendix section).The authors thank Piyalee Pal, Sciformix, A Covance Company, for providing medical writing support for development of the manuscript. The authors also thank Garima Joshi Sciformix, A Covance Company, for providing statistical support.
References
Footnotes
Contributors SSB contributed to the design, implementation and review of the study. SSD contributed to analysis of the results and writing of the manuscript.
Funding Development of this publication was financially supported by Sun Pharmaceutical Industries Ltd., India, through an independent medical writing grant.
Disclaimer The views and opinions described in this publication do not necessarily reflect those of the grantor.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.